The document provides information about the functions and organization of the cerebellum. It can be summarized as follows:
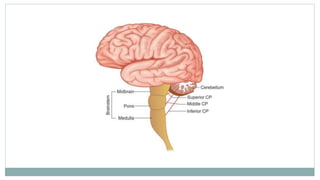
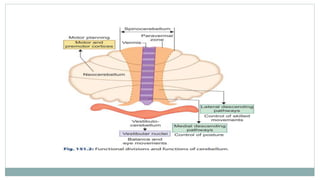
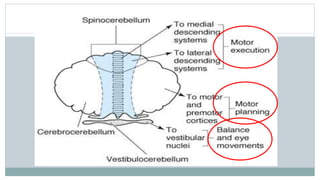
1. The cerebellum is divided into three lobes - vestibulocerebellum, spinocerebellum, and cerebrocerebellum - which are involved in balance, movement coordination, and planning/programming movements respectively.
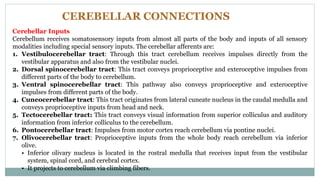
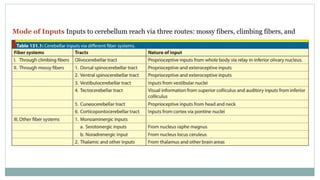
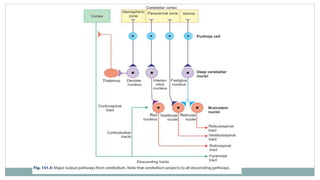
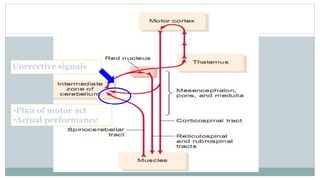
2. It receives various sensory inputs and projects to motor areas of the brainstem and cortex to integrate sensory and motor information and coordinate movement.
3. Damage to the cerebellum results in severe incoordination of movement and postural abnormalities due to its role in smoothing and regulating all aspects of movement.


























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


