Downloaded 75 times






















































![ Immittance is a physical characteristic of all
mechanical vibratory systems, of which the middle
ear is one example”
Immittance audiometry is an objective technique which
evaluates middle ear function by three procedures: ]
static immittance,
tympanometry, and
the measurement of acoustic reflex threshold sensitivity](https://image.slidesharecdn.com/hearingtest-210708040338/85/Hearing-tests-67-320.jpg)















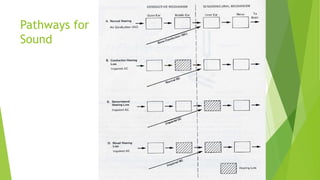
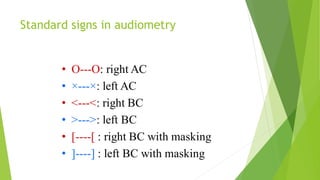
The document discusses human ear tests of hearing. It describes three main types of hearing loss - conductive, sensorineural, and mixed - and explains what each type is caused by. It also outlines several common tuning fork tests used to evaluate hearing, including Rinne's test, Weber test, and Schwabach test. Finally, it provides an overview of pure tone audiometry testing procedures and how to interpret audiogram results.

















































































