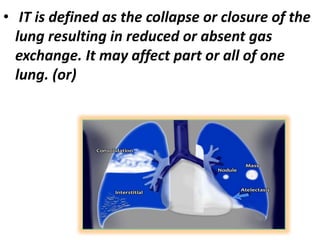
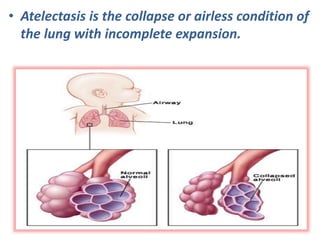
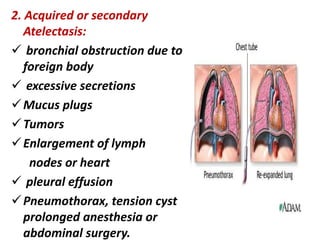
Atelectasis is the collapse or closure of part or all of the lung resulting in reduced gas exchange. It can be primary, due to prematurity or lung immaturity, or secondary due to obstruction from mucus, tumors, or surgery. Symptoms include rapid shallow breathing, cough, hypoxia, and fever. Diagnosis involves chest x-ray, sputum tests, and CT scans. Treatment focuses on positioning, suctioning mucus, oxygen therapy, and preventing infections. Nursing care manages breathing, airway clearance, gas exchange, and monitors for complications like infections.