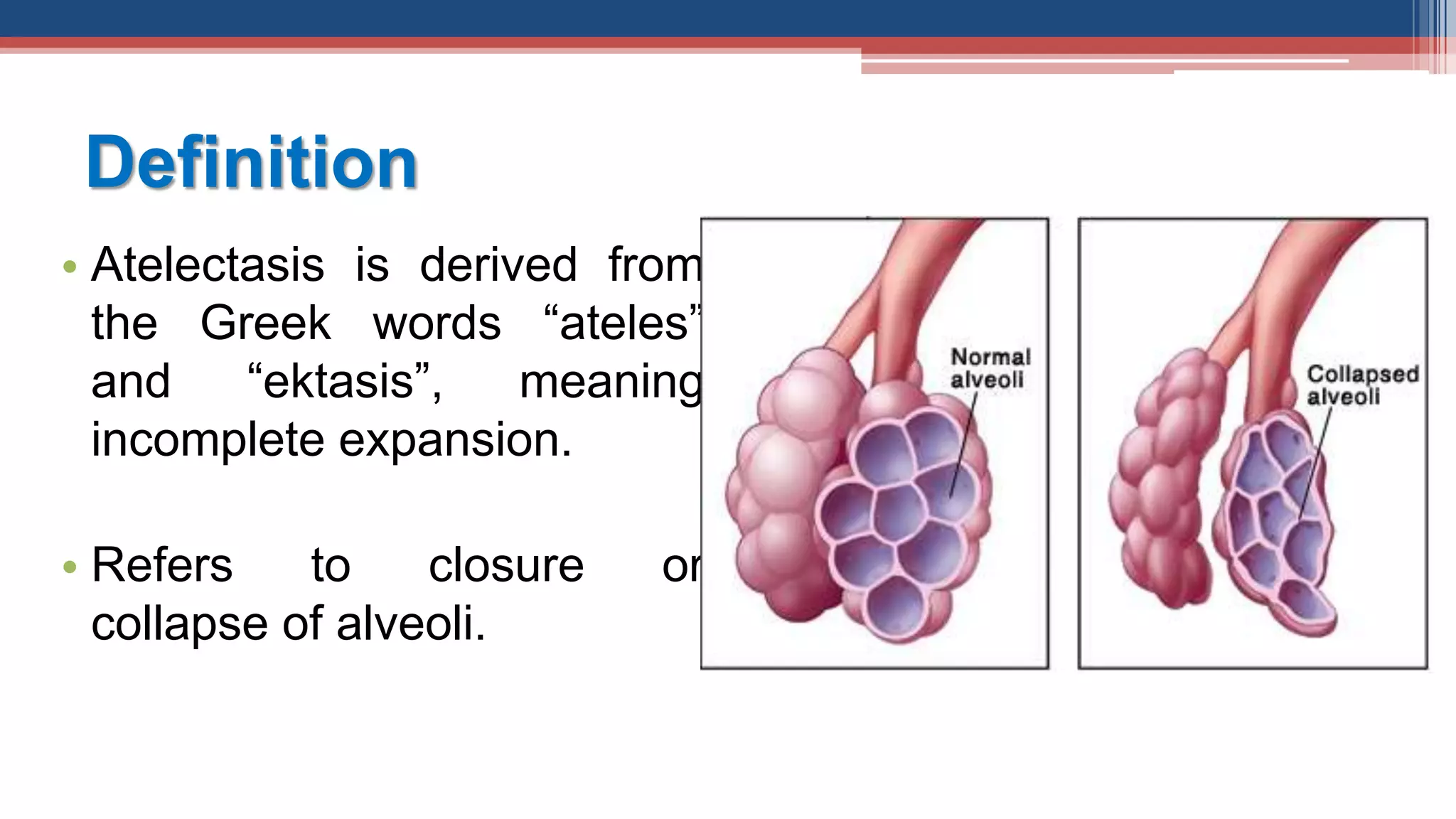
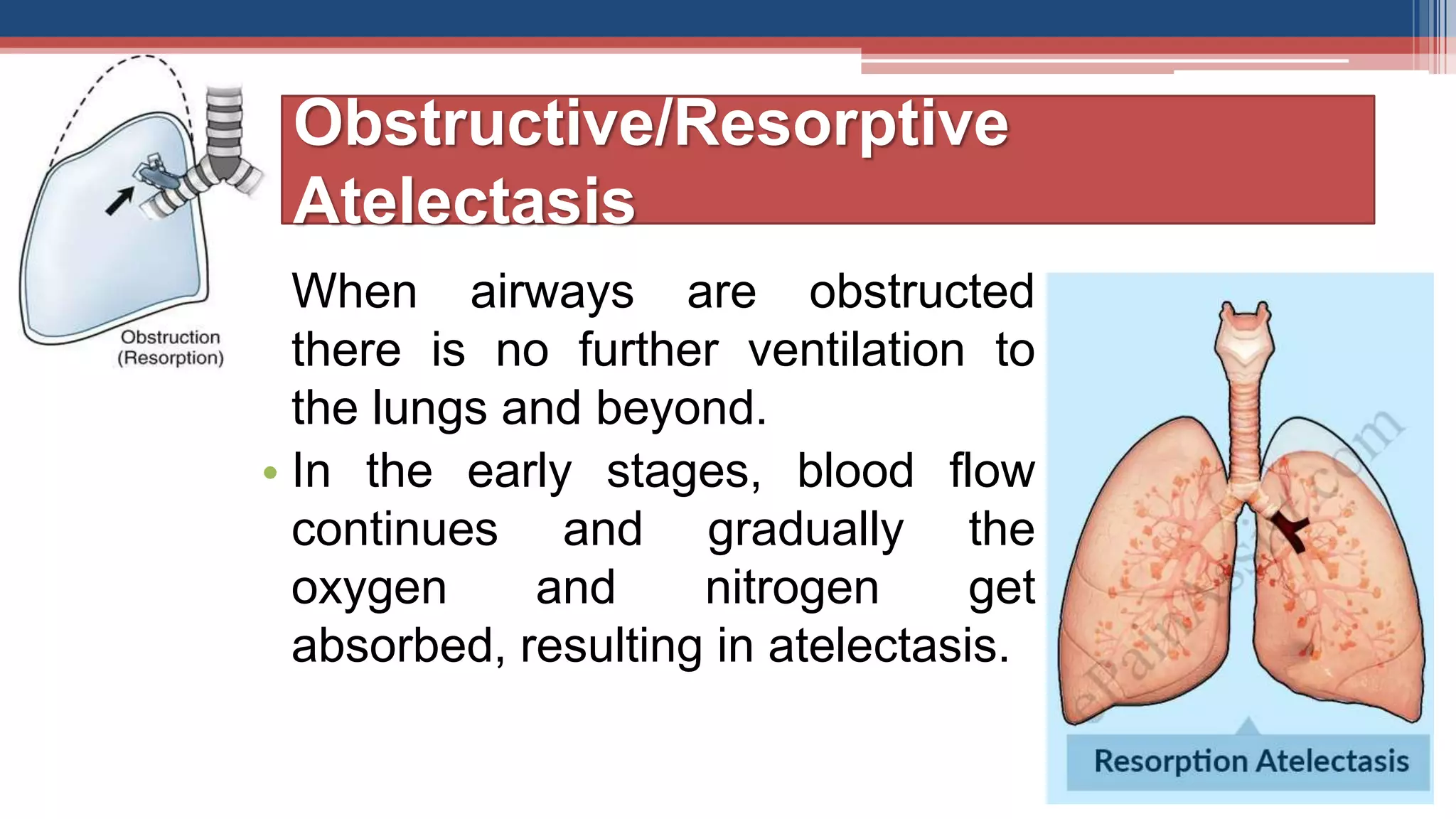
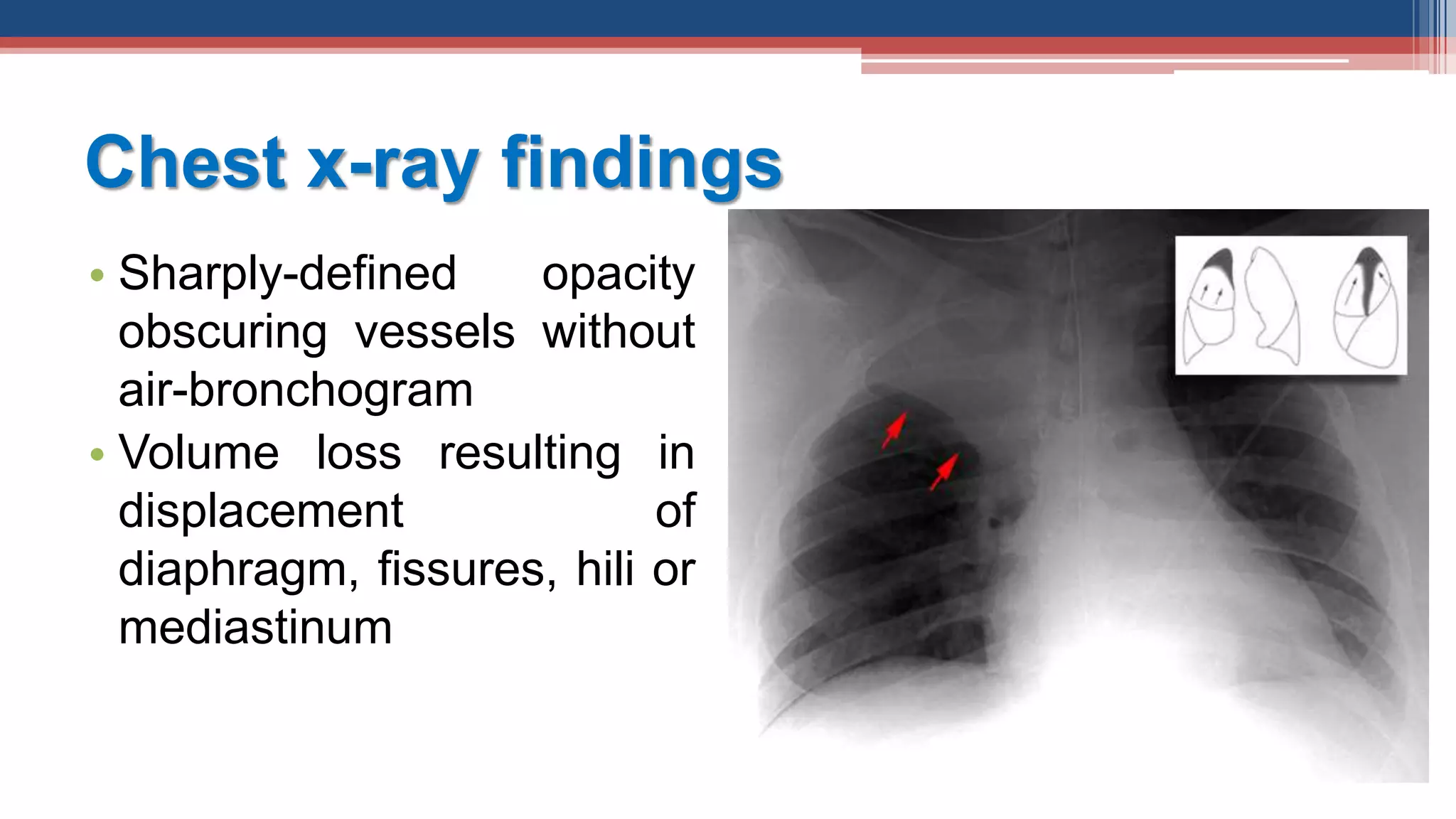
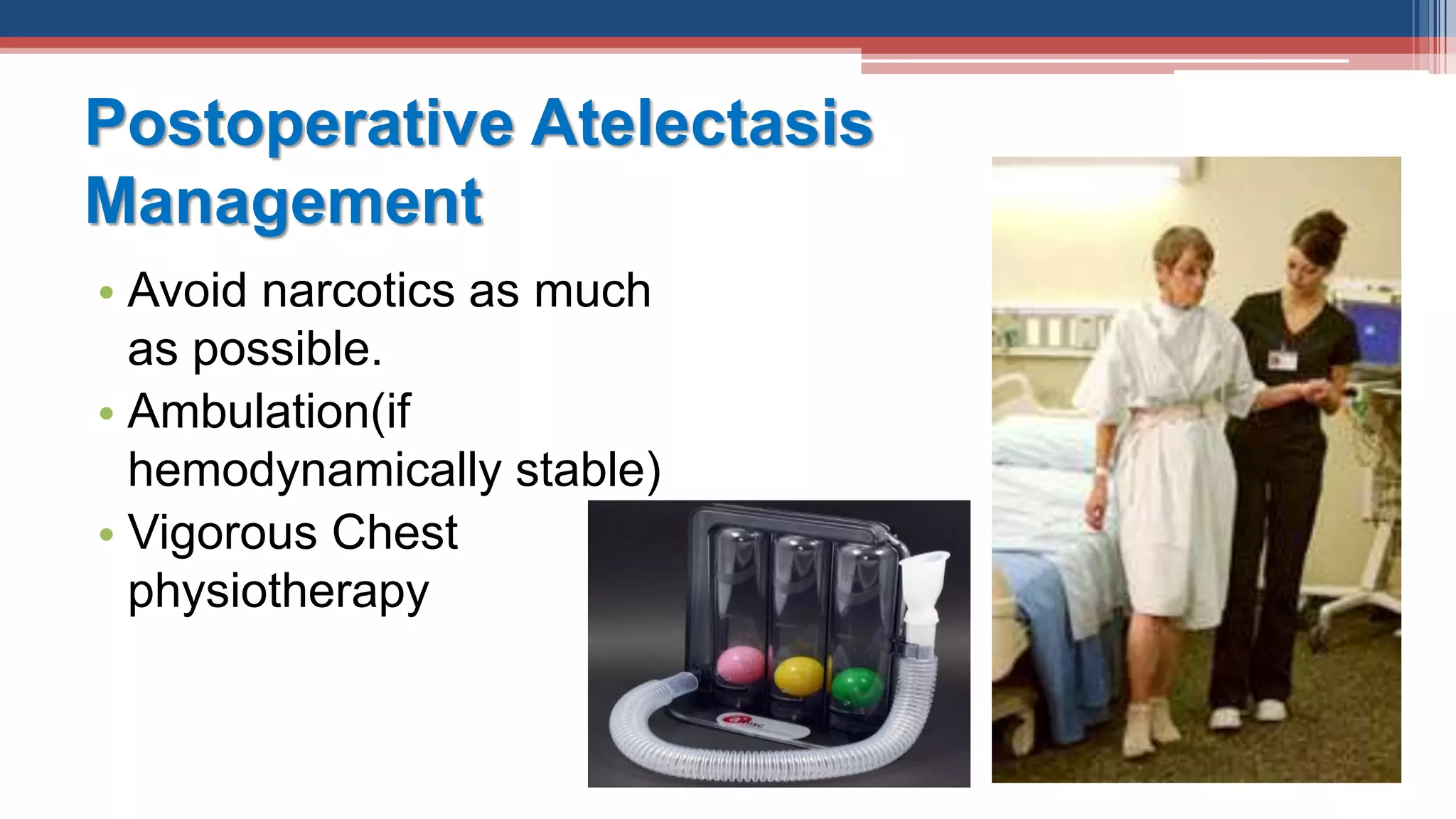
This document discusses atelectasis, which is the collapse or closure of alveoli in the lungs. It defines atelectasis and reviews its causes, types, symptoms, diagnosis, and treatment. Atelectasis can be obstructive or non-obstructive, acute or chronic. Risk factors include smoking and general anesthesia. Diagnosis involves chest x-ray, pulse oximetry, and arterial blood gas analysis. Treatment focuses on treating the underlying cause, chest physiotherapy, bronchodilators, surgery if needed, and preventing complications like pneumonia. Nursing care involves airway clearance techniques and strategies to improve ventilation and gas exchange.