Download as PPSX, PPTX



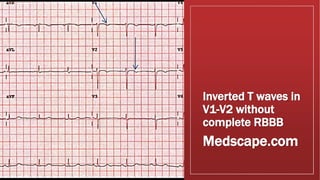
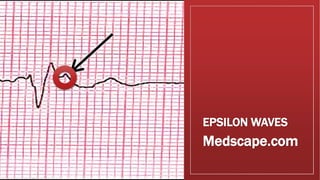
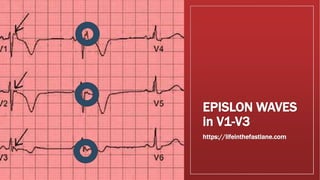
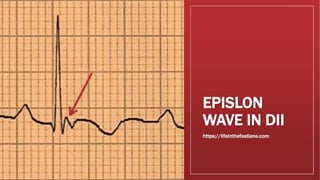

Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) is an inherited heart muscle disease characterized by structural abnormalities and fatty replacement of the right ventricle muscle leading to ventricular arrhythmias. It is an important cause of sudden cardiac death in young adults. The disease results from genetic mutations that cause programmed cell death and fibrosis of the right ventricle muscle. Diagnosis is based on ECG findings like inverted T-waves in the right ventricle leads and epsilon waves, along with imaging showing right ventricle structural changes. Treatment involves medications like beta-blockers and implantable defibrillators to prevent arrhythmias.





































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















