Introduction
• Arrhythmogenic rightventricular cardiomyopathy (ARVC),
also referred to as arrhythmogenic right ventricular dysplasia
(ARVD) or simply arrhythmogenic cardiomyopathy
• Is a heritable heart muscle disorder that predominantly affects
the right ventricle.
• Progressive loss of right ventricular myocardium (occasionally
left ventricle) and its replacement by fibrofatty is the
pathological hallmark of the disease.
• Common causes of sudden cardiac death in young patients.
4.
EPIDERMIOLOGY
• The estimatedpopulation prevalence is thought to range
around 1 in 1000-5000
• It typically presents in young individuals.
• Slightly male predominance (M:F 2.7:1)
• Familial occurrence of ARVC of about 30-50%, with mainly
autosomal dominant inheritance.
• ARVC accounts for 3–4% of deaths in sports
5.
Clinical presentation
• Palpitations
•Syncope
• Sudden cardiac arrest
• Jugular venous distension
• Hepatic congestion
• Symmetric, pitting pedal edema
• Exercise intolerance
• Exertion is a common trigger for the causative ventricular
tachyarrhythmias.
6.
Diagnosis
• The diagnosisof ARVC is based on established criteria
determined by a task force comprising the European Society
of Cardiology and the International Society and Federation of
Cardiology.
• The diagnosis of ARVC is based on the presence of two major
criteria, one major and two minor criteria or four minor
criteria encompassing structural, histologic,
electrocardiographic, arrhythmic, and genetic factors
proposed.
7.
Major criteria
• Globalor regional dysfunction and structural alterations:
– Severe dilatation of the right ventricle (RV) and reduced RV ejection
fraction
– Severe segmental dilatation of the RV
– Localized RV aneurysm
• Tissue characterization:
– Fibrofatty replacement of the RV myocardium (endocardial biopsy)
• Depolarization or conduction abnormalities:
– Epsilon waves
– Prolonged QRS complex (>110msec) in V1-V3
• Family history:
– Familial disease confirmed at autopsy or surgery
8.
Minor criteria
• Globalor regional dysfunction and structural alterations:
– Mild dilatation of the right ventricle (RV) and reduced RV ejection fraction
– Mild segmental dilatation of the RV
– Regional RV hypokinesia
• Repolarization abnormalities:
– Inverted T waves (V2-V3)
• Depolarization or conduction abnormalities:
– Late potentials
• Arrhythmias:
– Ventricular tachycardia with LBBB and frequent VES
• Family history:
– Family history of sudden death due to suspected ARVC
– Family history of ARVC on diagnostic criteria
9.
Radiographic features
• Plainradiograph
• Chest radiographic findings are non-specific and can often be
normal. May show evidence of right ventricular dilatation (best
seen on a lateral
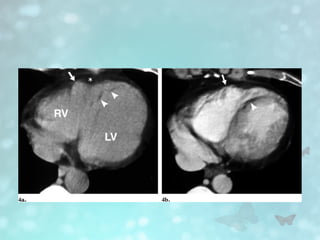
• CT
• May show right ventricular dilation and fatty low attenuation to
the right ventricular wall.
11.
• Echocardiography
• Echocardiographyhas inconsistent sensitivity and specificity
for the diagnosis of ARVC and is not considered a primary
modality in the final diagnosis
• Supportive features include:
• Disproportionate enlargement of the basal right ventricle
• Secondary ("functional") tricuspid regurgitation
– associated with right ventricular dilatation and dysfunction
• Intensely echogenic moderator band
13.
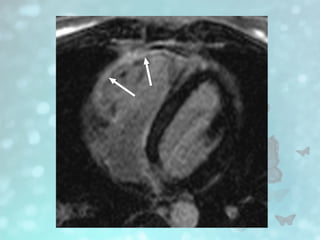
• MRI
• CardiacMRI is the most sensitive diagnostic imaging
modality.
• Increased myocardial right ventricle (RV) signal suggesting
fatty infiltration
• Focal wall motion abnormalities
• Increased right ventricular volumes with quantification,
dilatation of the RV and right ventricular outflow tract (RVOT),
thinning of the right ventricular wall.
• Delayed myocardial enhancement suggesting fibro-fatty
replacement
14.
• Major cardiacMRI diagnostic criteria are:
• Regional RV akinesia or dyskinesia or dyssynchronous RV
contraction and 1 of the following:
– ratio of RV end-diastolic volume to BSA (body surface area)
≥110 mL/m2
(male) or ≥100 mL/m2
(female)
– RV ejection fraction ≤40%
• Minor cardiac MRI diagnostic criteria are:
• Regional RV akinesia or dyskinesia or dyssynchronous RV
contraction and 1 of the following:
– ratio of RV end-diastolic volume to BSA ≥100 to <110
mL/m2
(male) or ≥90 to <100 mL/m2
(female)
– RV ejection fraction >40% to ≤45%
Treatment
• Treatment ofARVC aims to prevent sudden cardiac death.
Treatment options include avoidance of strenuous exercise and
competitive sports or training, β blockade, antiarrhythmic
medications, catheter ablation , implantable cardioverter
defibrillator therapy , and cardiac transplant.
23.
REFERENCES
• Weerakkody Y,Campos A, Carroll D, et al. Arrhythmogenic
right ventricular cardiomyopathy. Reference article,
Radiopaedia.org (Accessed on 19 Mar 2025)
https://doi.org/10.53347/rID-7439
• Cardiac MRI in Arrhythmogenic Right Ventricular Cardiomyopathy.
Darra T. Murphy, Suzanne C. Shine, Andrea Cradock, Joseph M.
Galvin, Edward T. Keelan, and John G. Murray.American Journal of
Roentgenology 2010 194:4, W299-W306
• Radswiki T, Knipe H, Tatco V, et al. Arrhythmogenic right
ventricular cardiomyopathy diagnostic criteria. Reference article,
Radiopaedia.org (Accessed on 19 Mar 2025)
https://doi.org/10.53347/rID-11144
Editor's Notes
#5 Why it is called arrythmogenic because it is characterized by abnormal heart rhythm which can lead above symtoms
#7 Epsilon wave-small positive deflection at the end of QRS complex best seen on the right precordial lead V1-V3.
#8 Late potential –abnormal electrical signal occur at the end of QRS complex indicate delay conduction in the ventricle.
VES-Ventricular exctra systole
#10 Unenhanced (a) and contrast-enhanced (b) CT scans show slight bulging of the anterior wall of the right ventricle (RV ) (arrow) probably
In addition, fatty tissue is seen in the right ventricular aspect of the subendocardial portion of the ventricular septum (arrowheads).
#14 Akinesia-no movement , dyskinesia- abnormal movement usually paradoxical out word movent. Dyssincronous- different segment not contracting at same time
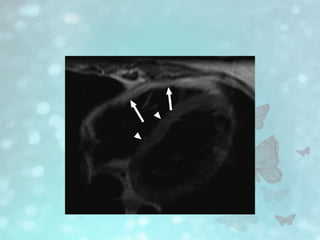
#15 Black blood breath-hold T1-weighted MR image shows diffuse fatty infiltration of right ventricle. Note increased signal intensity from fat in free wall of right ventricle (arrows), compared with intermediate signal intensity from septum and left ventricular wall (arrowheads)
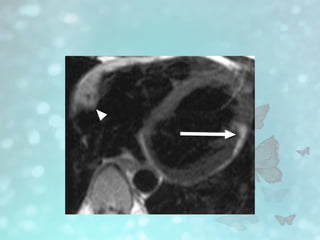
#16 T1-weighted MR image shows fat infiltration of both ventricles. There is diffuse fat within right ventricular free wall (arrowhead) in addition to focal fat in left ventricular wall (arrow). Fatty infiltration of both ventricles is rare in arrhythmogenic right ventricular cardiomyopathy.
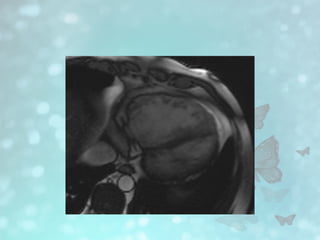
#17 True fast imaging with steady-state precession image shows aneurysm formation of right ventricular wall (arrow)
#18 . True fast imaging with steady-state precession image in systole shows marked dilatation of right ventricle. These findings satisfy two major diagnostic criteria for arrhythmogenic right ventricular cardiomyopathy
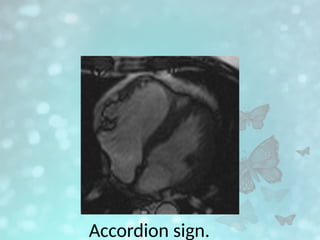
#19 True fast imaging with steady-state precession MR images in long axis show right ventricular aneurysm, with corrugated right ventricular wall (accordion sign), and dyskinesia.