Downloaded 31 times

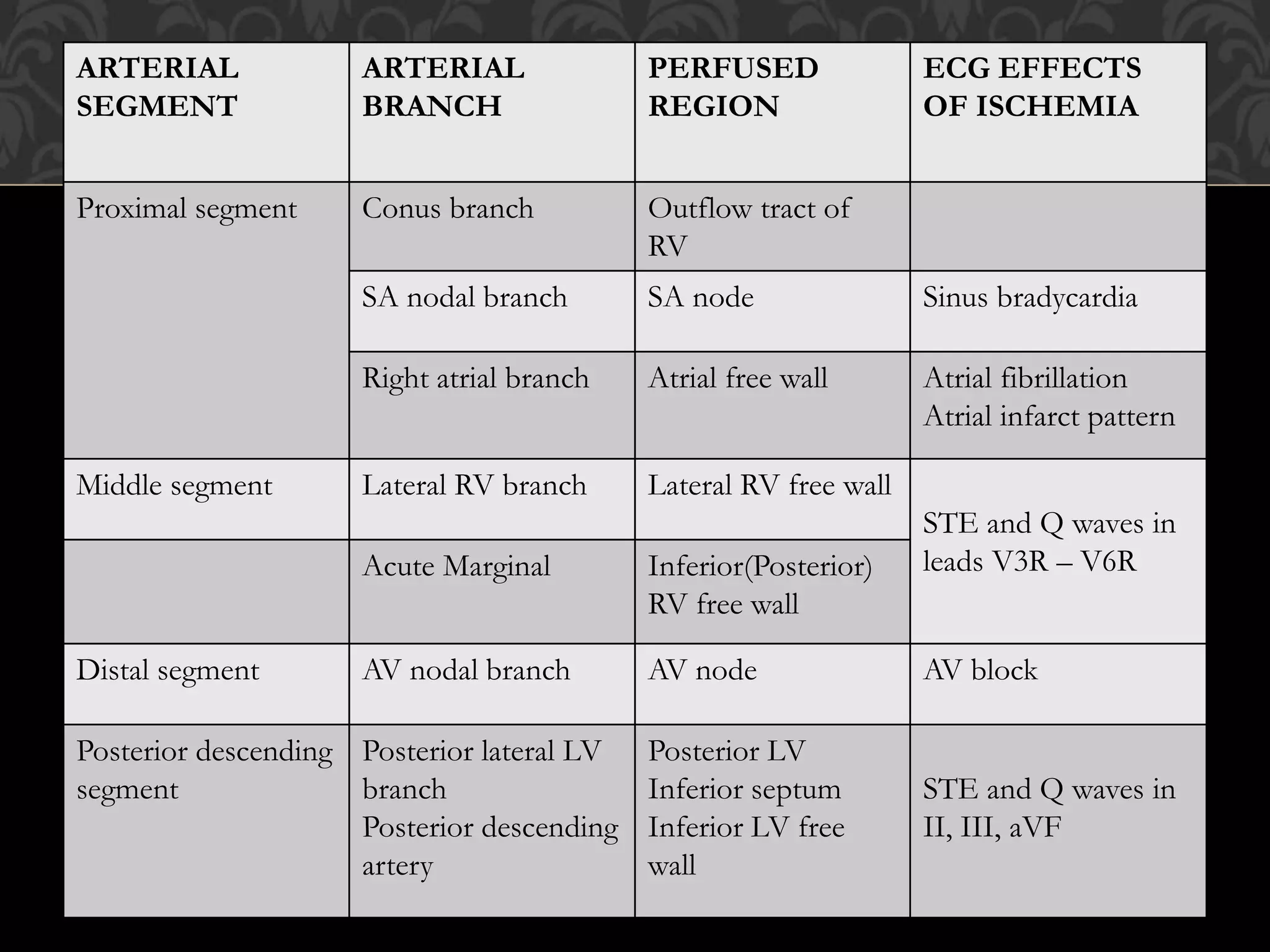


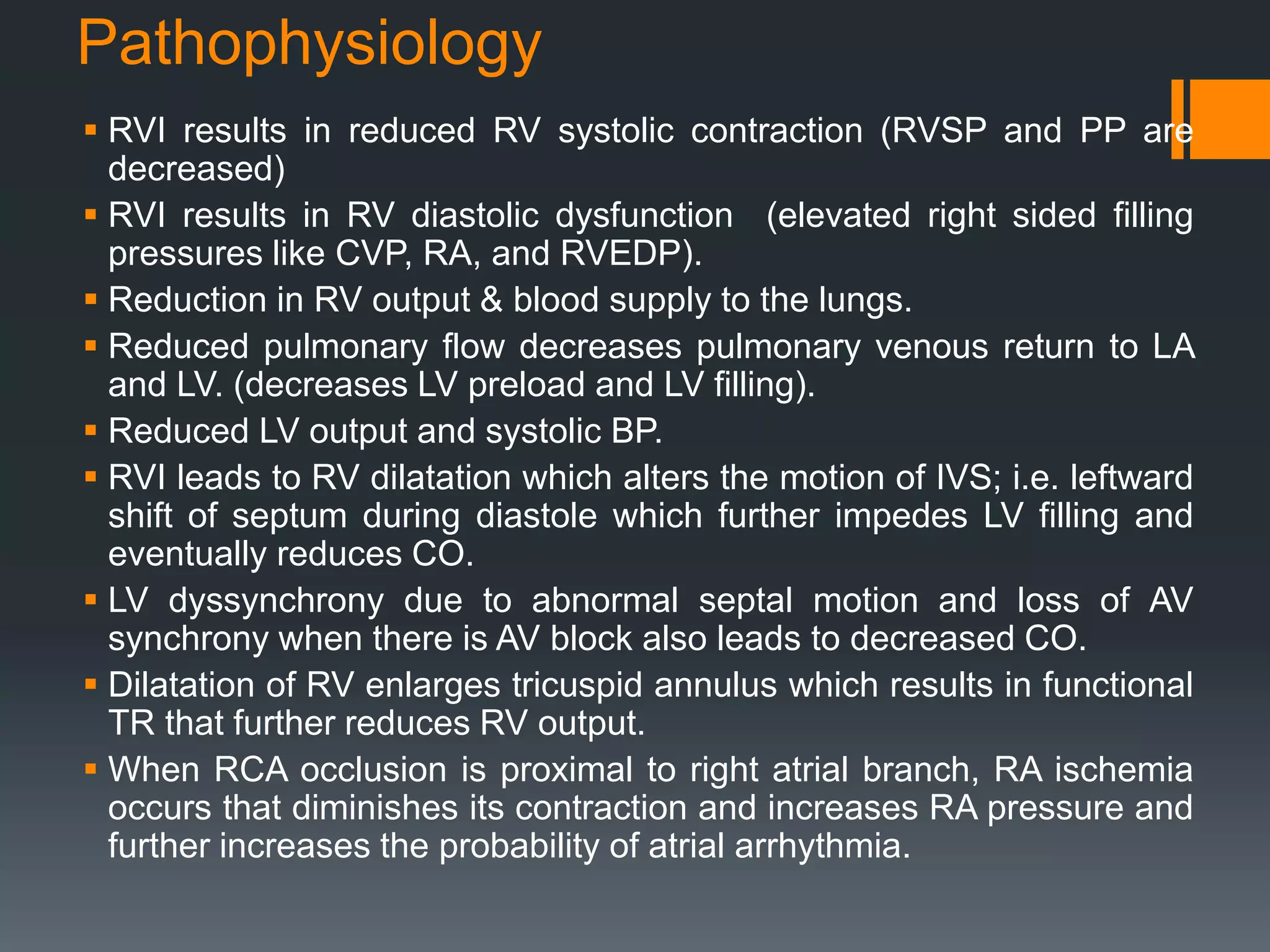
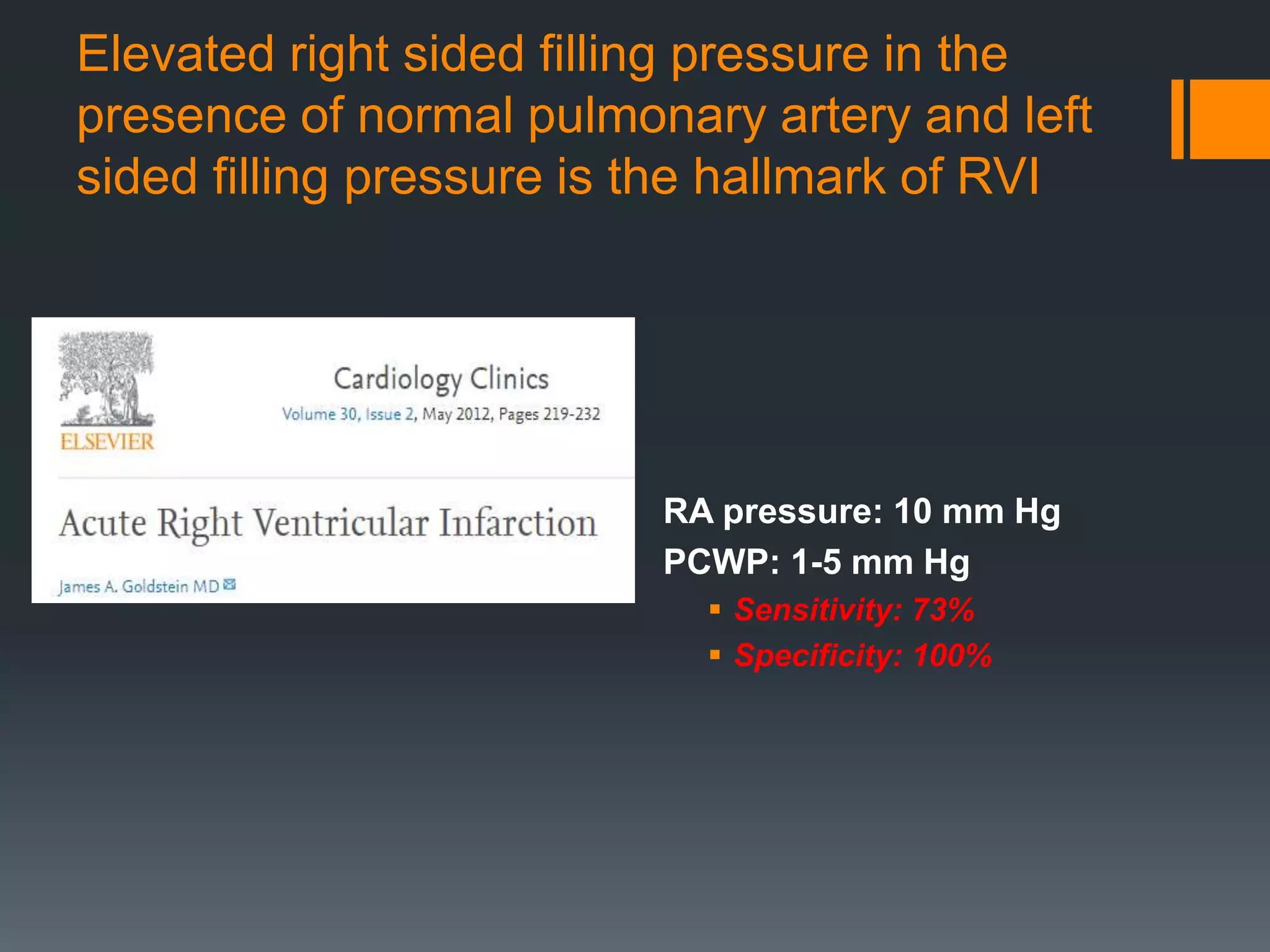
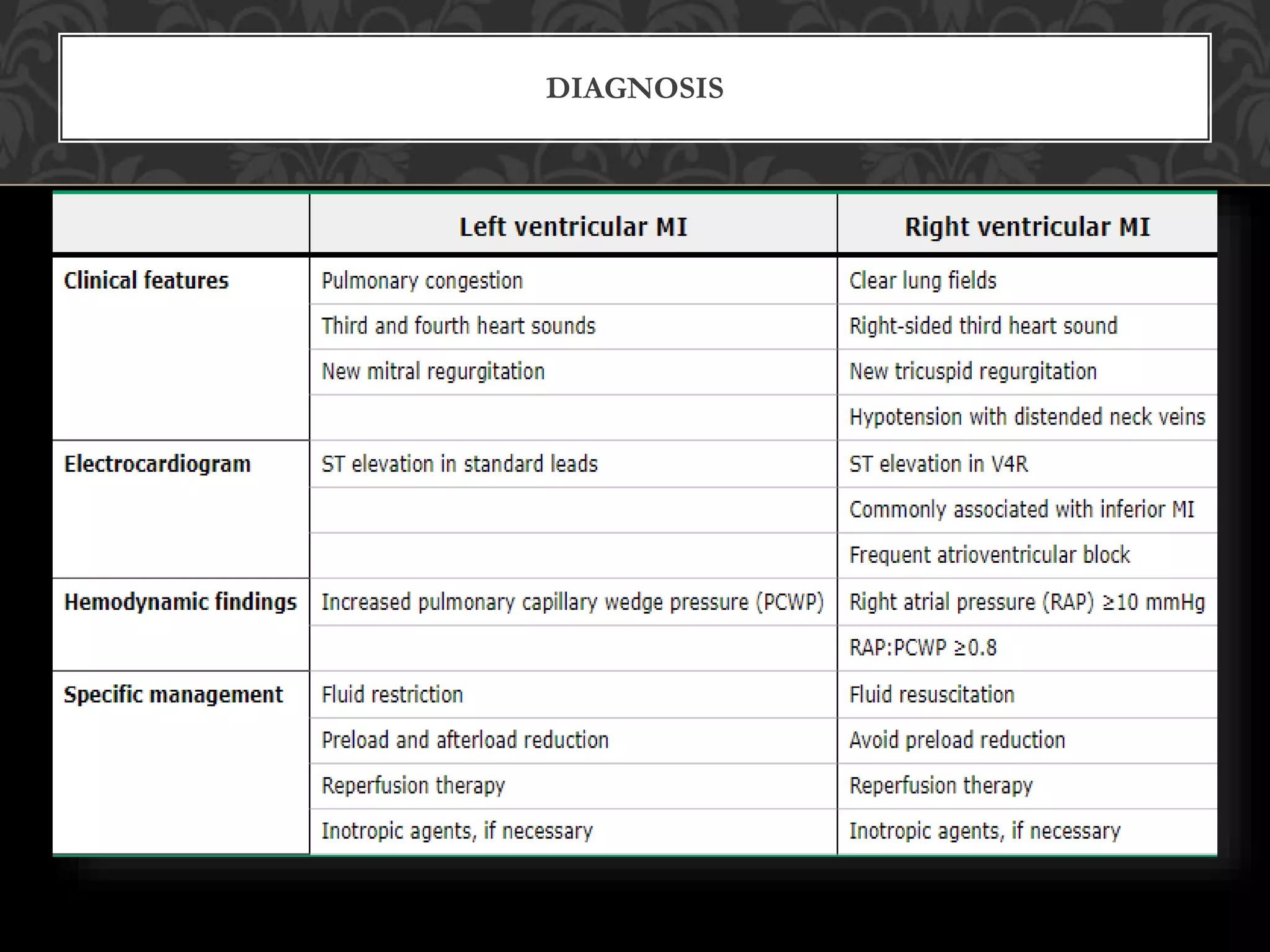
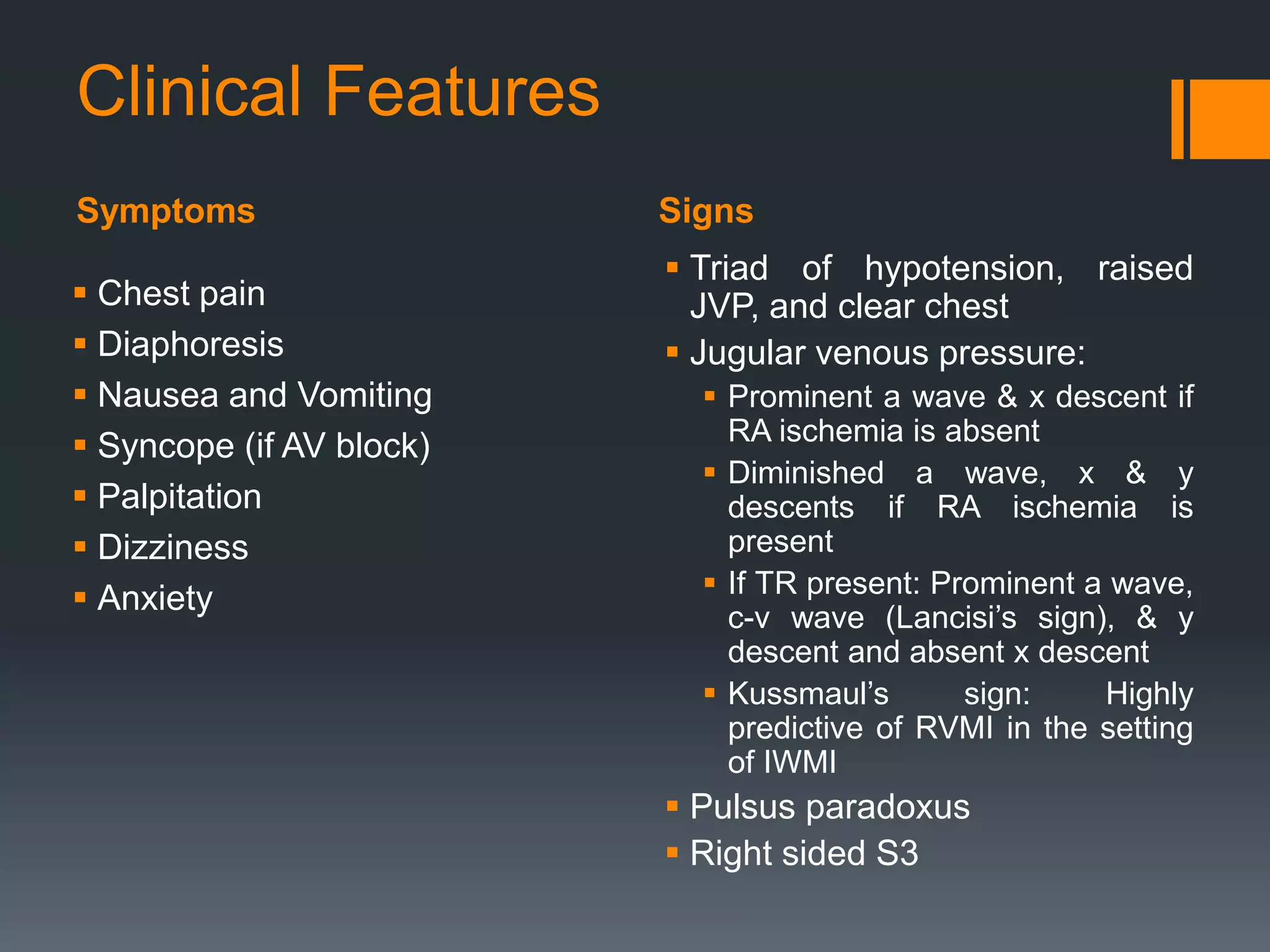
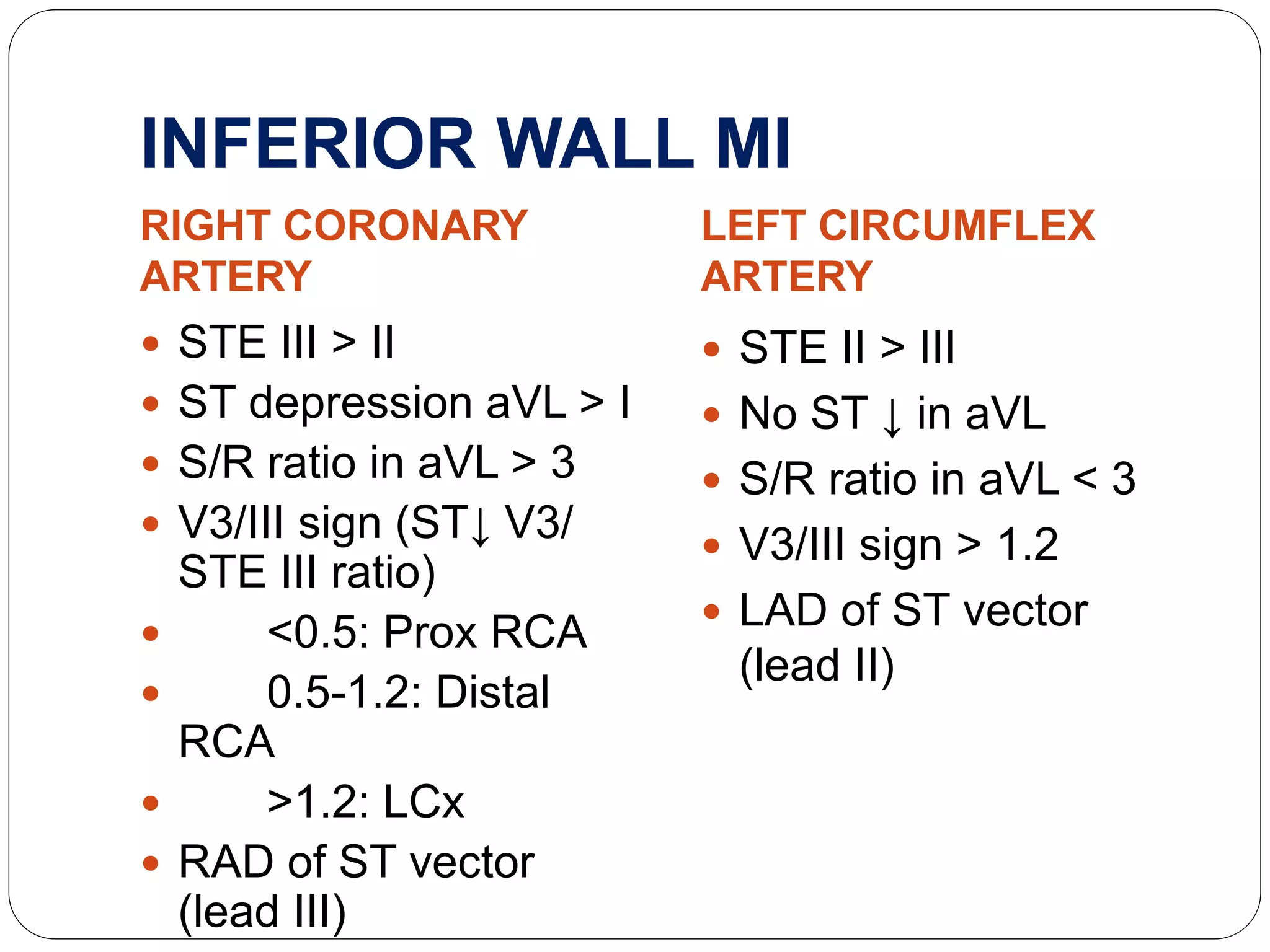
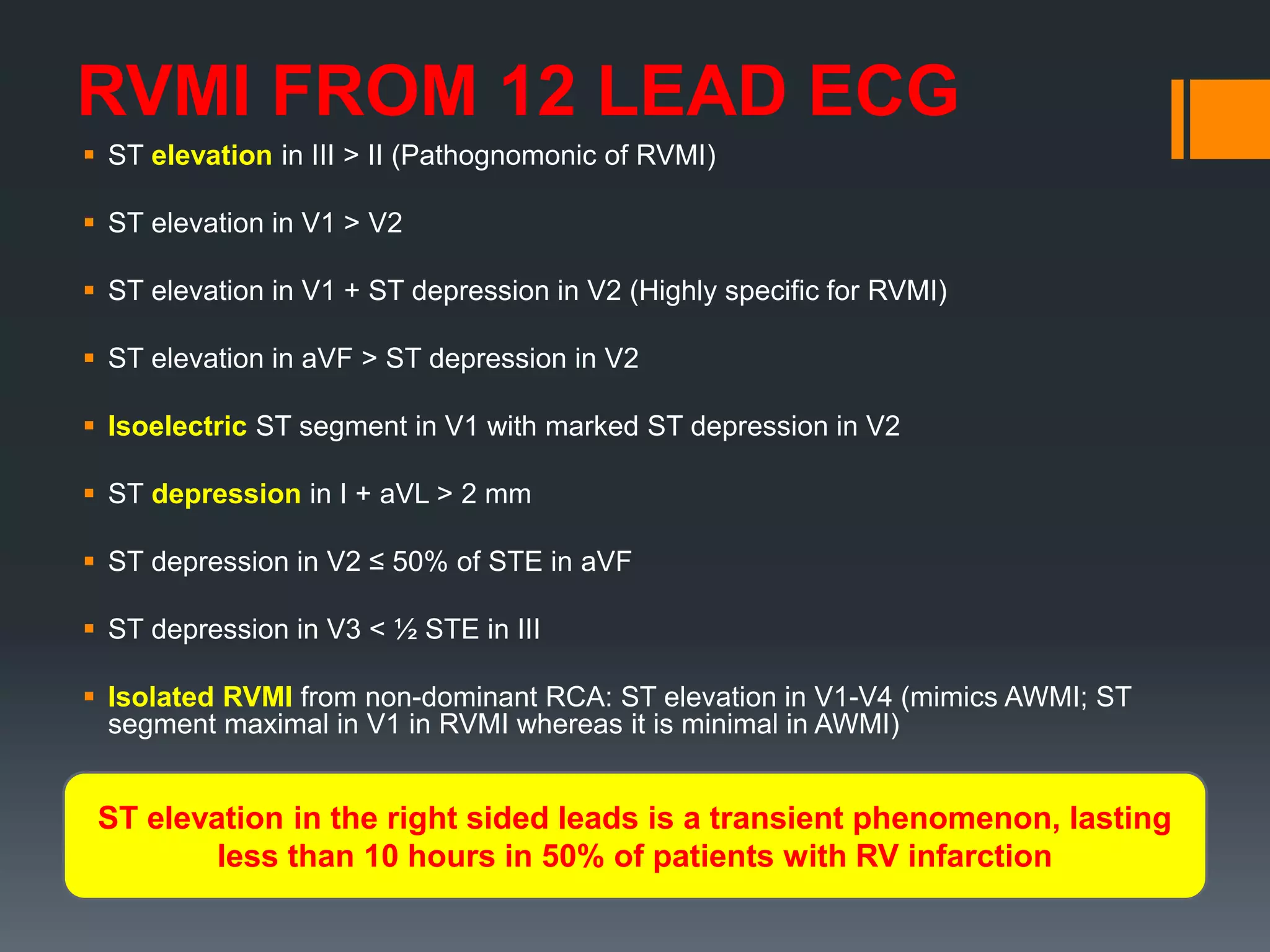
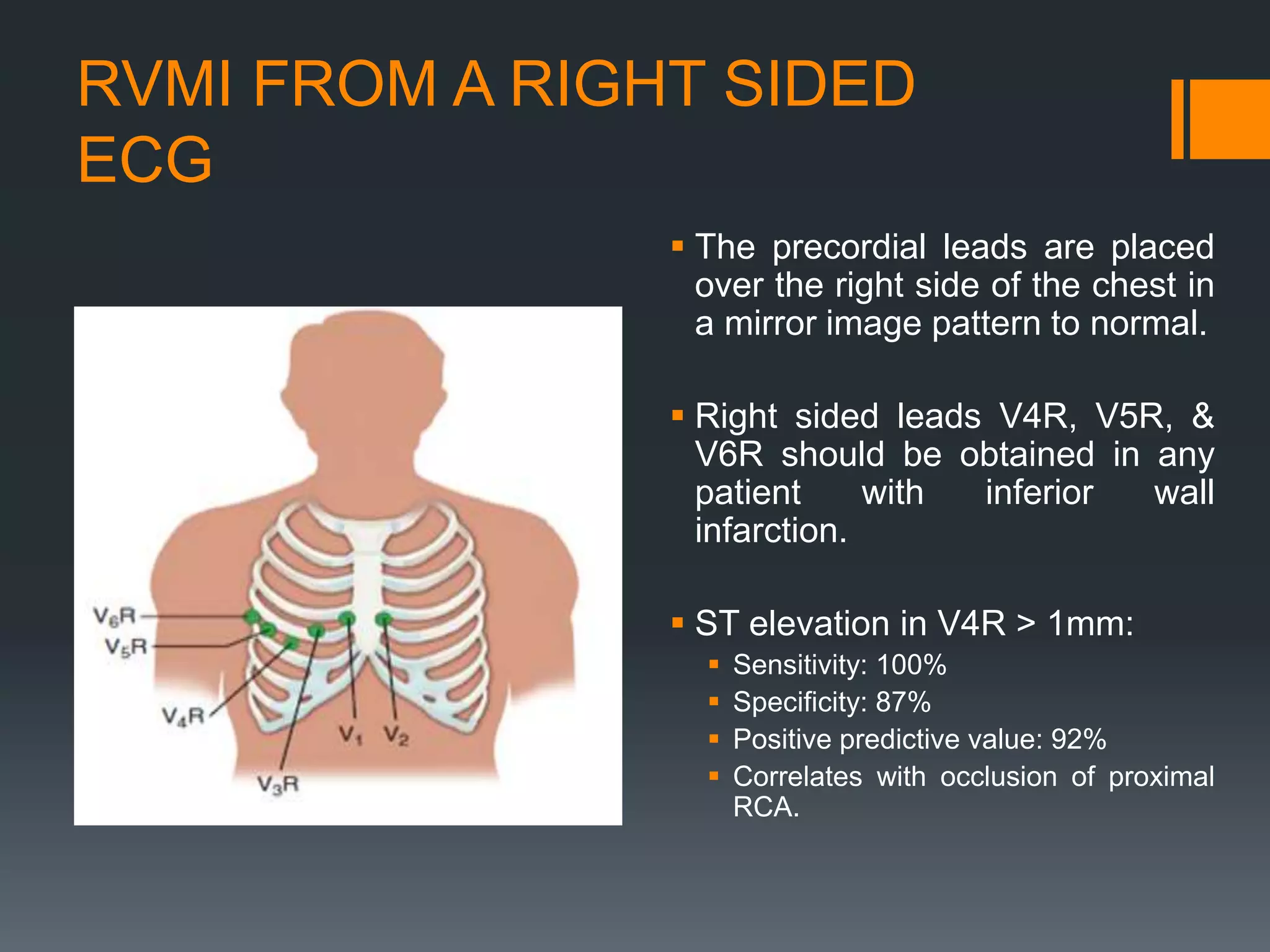



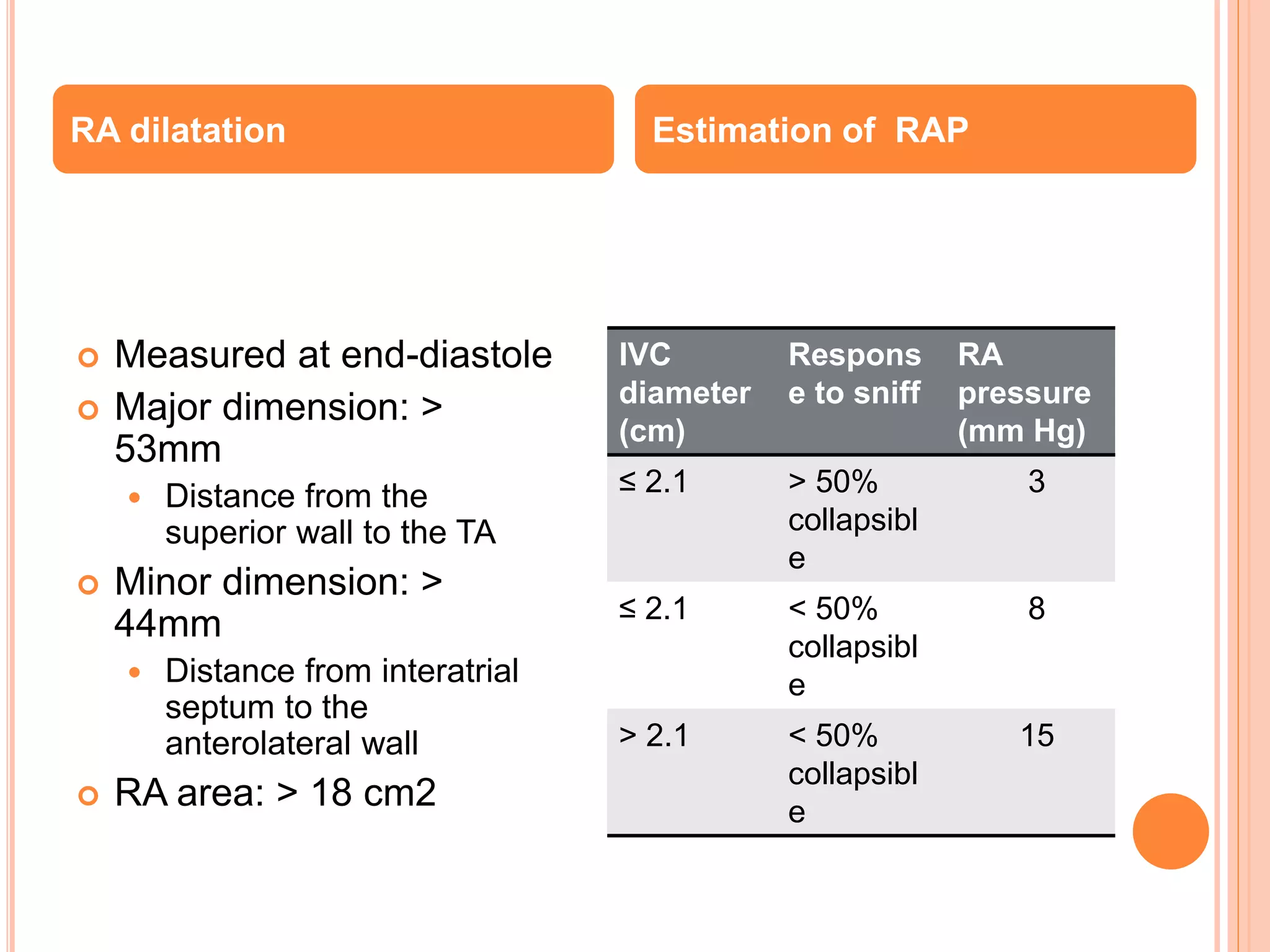
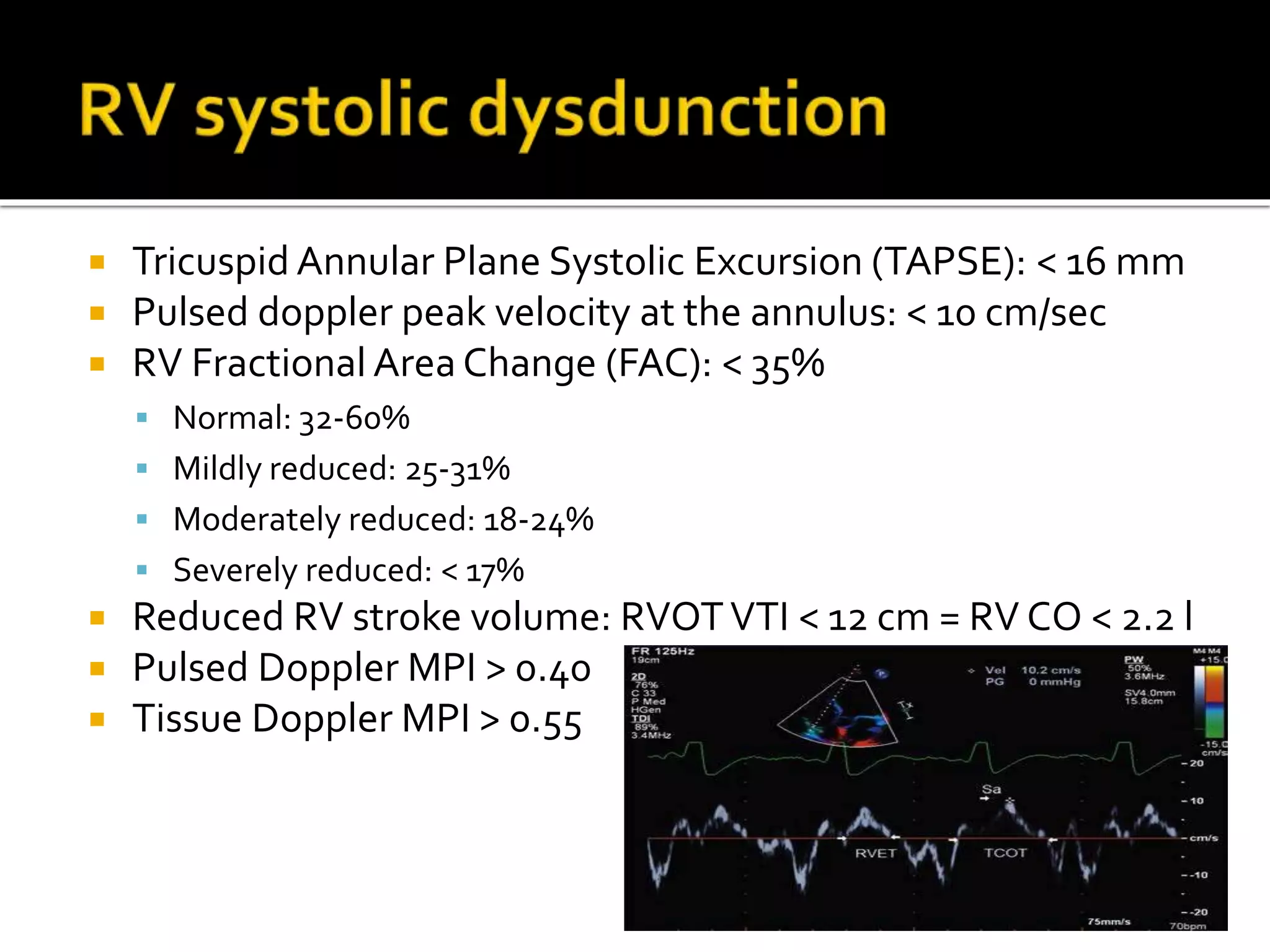
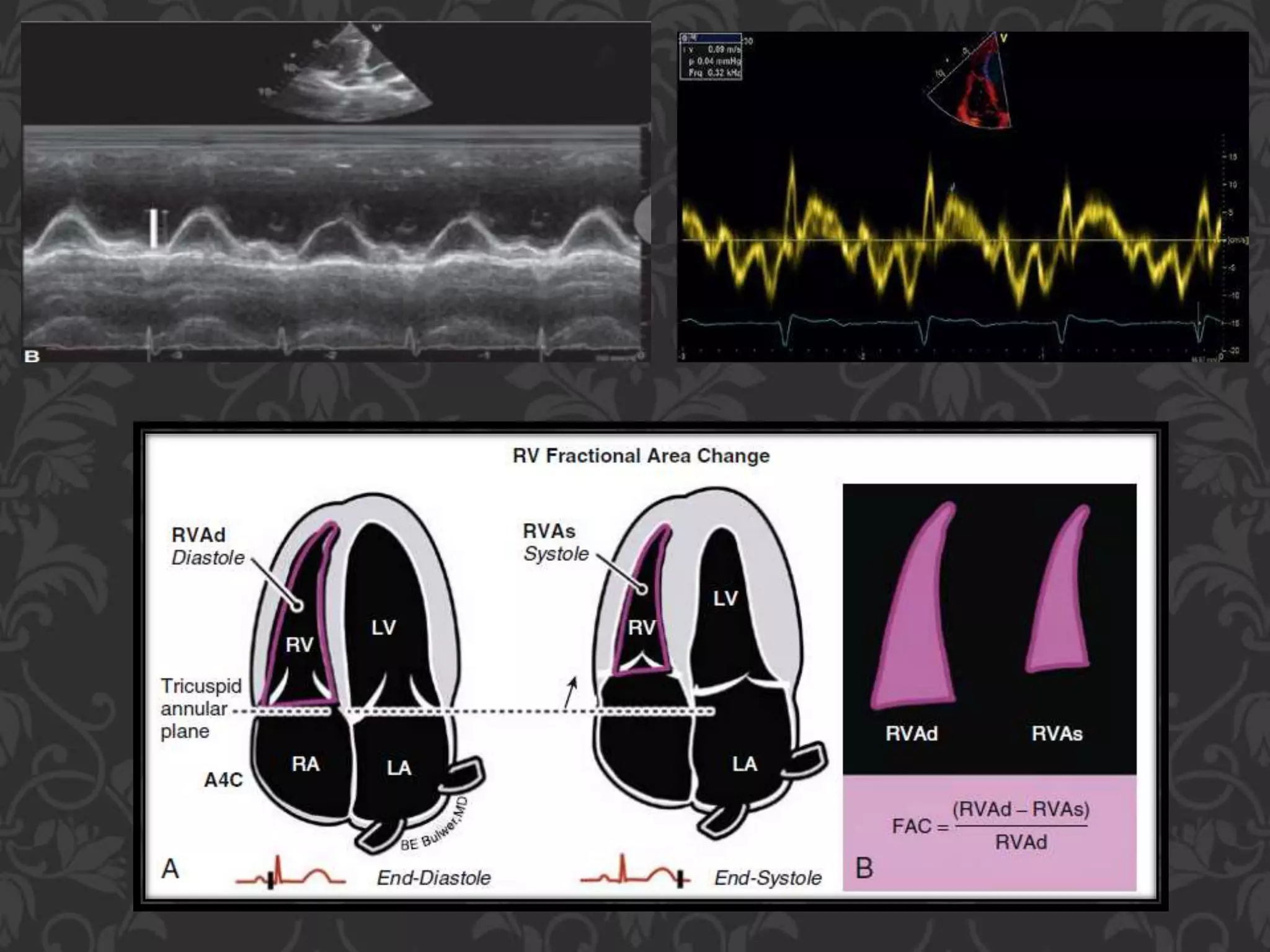
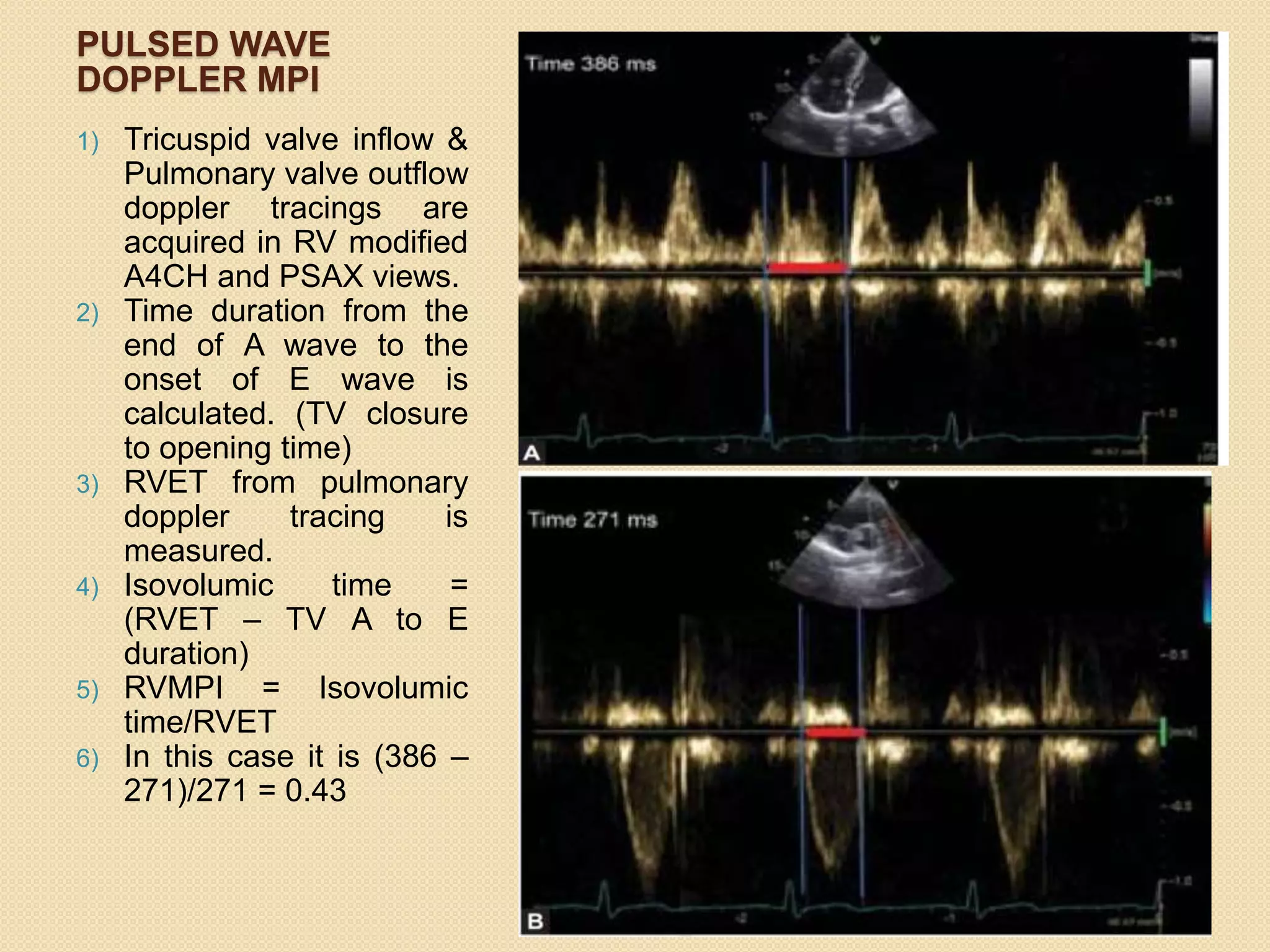




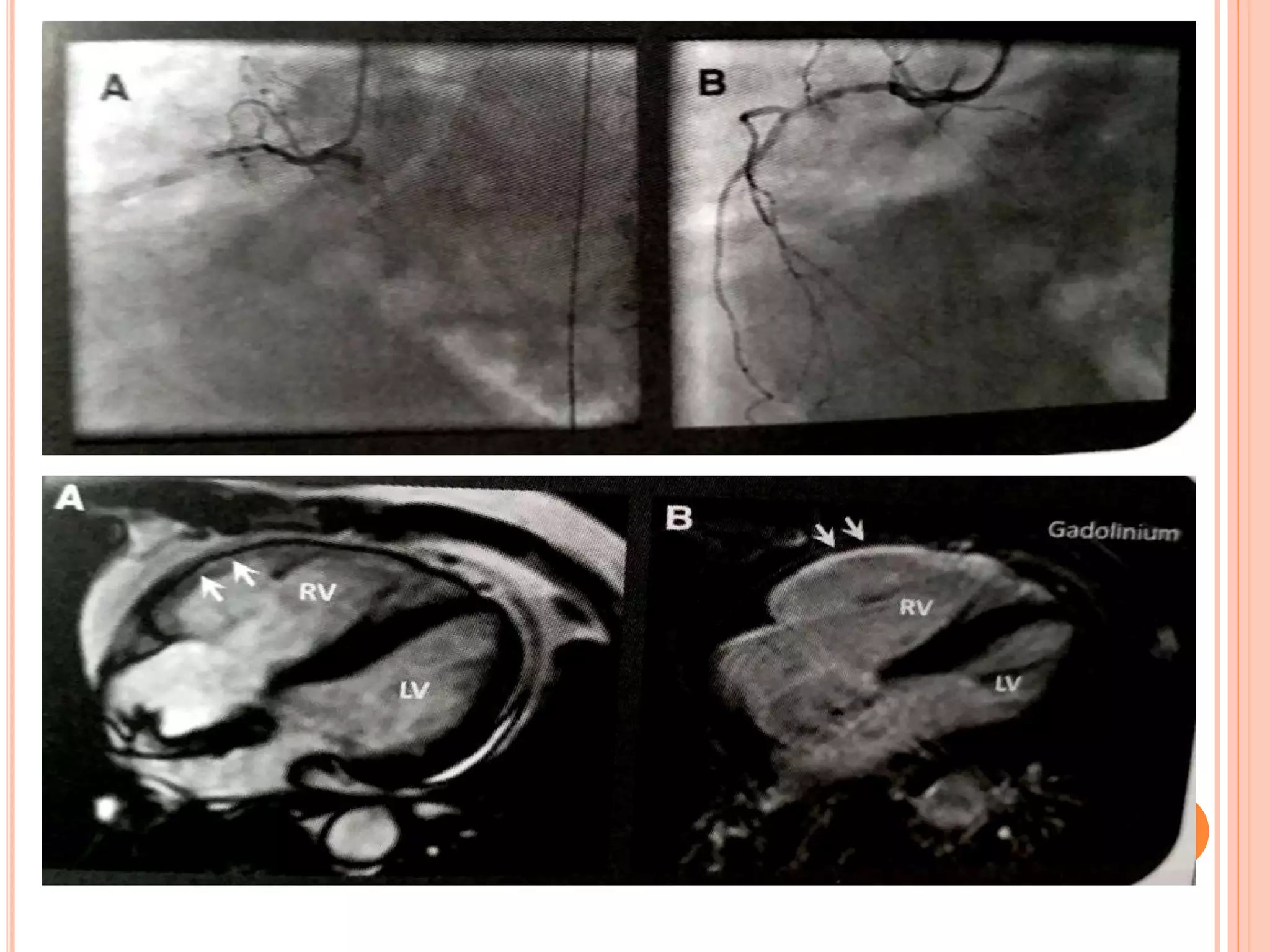


This document discusses right ventricular myocardial infarction (RVMI). Some key points: 1. RVMI occurs in 30-50% of inferior wall ST-elevation MIs and 3-5% of MIs are isolated RVMI. 2. RVMI is associated with higher morbidity and mortality than LV MI due to hemodynamic and electrical complications in around 50% of cases. 3. Diagnosis of RVMI can be made based on ECG findings of ST elevation in leads V1-V3 and III>II, and echo findings of RV dilation, hypokinesis of the RV free wall, and elevated right-sided pressures. 4. Management of RVMI focuses on optimizing RV












































































