Downloaded 22 times

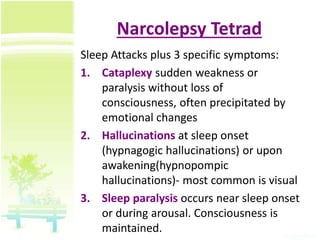
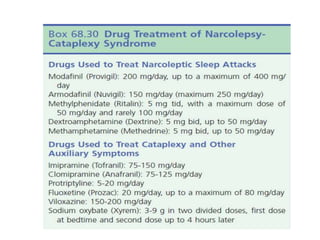
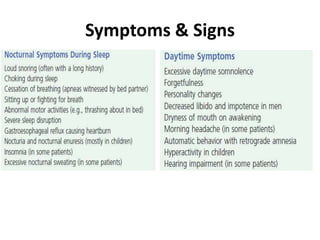


Sleep disorders can be classified into six main categories. Narcolepsy is characterized by excessive daytime sleepiness and irregular sleep-wake cycles. It is caused by a lack of hypocretin in the brain and symptoms include sleep attacks, cataplexy, hallucinations, and sleep paralysis. Obstructive sleep apnea is the most common breathing-related sleep disorder and involves repetitive collapse of the upper airway during sleep causing fragmented sleep and oxygen deprivation. Parasomnias are abnormal behaviors that occur during sleep like sleepwalking, nightmares, and REM sleep behavior disorder. Restless legs syndrome involves unpleasant sensations in the legs when trying to fall asleep that are relieved by movement. Polysomnography and the

























































![Icsdsleepdisorders Pgs[1]](https://cdn.slidesharecdn.com/ss_thumbnails/icsdsleepdisorderspgs1-12709357520571-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Sleep disorders [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/sleepdisordersautosaved-180531135608-thumbnail.jpg?width=640&height=640&fit=bounds)
































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









