Downloaded 851 times
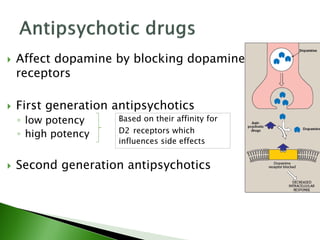


Antipsychotic drugs are primarily used to treat schizophrenia and other psychotic disorders by reducing hallucinations, delusions, and other positive symptoms. They are categorized into first-generation antipsychotics that are associated with movement disorders, and second-generation antipsychotics that have fewer extrapyramidal side effects but higher risks of metabolic adverse effects. While antipsychotics do not cure schizophrenia, they can help control symptoms and allow patients to function better with support. Long-term maintenance treatment is often required to prevent relapse of psychotic episodes.








































































































