Downloaded 24 times
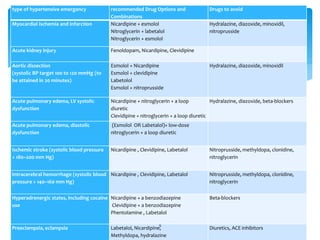
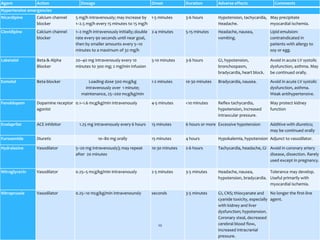
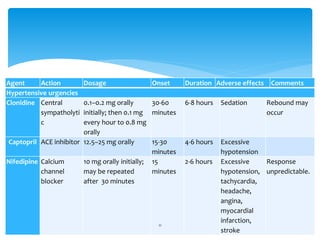

The document discusses hypertensive urgencies and emergencies. It defines hypertensive urgency as severe hypertension without acute end-organ damage, requiring blood pressure reduction within hours. Hypertensive emergency involves both severe hypertension and acute end-organ damage, requiring rapid blood pressure reduction within 1 hour to prevent serious morbidity or death. The document provides guidelines for evaluating and diagnosing these conditions, goals for reducing blood pressure, drug options for specific types of hypertensive emergencies, and subsequent oral therapy once the emergency is resolved.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





