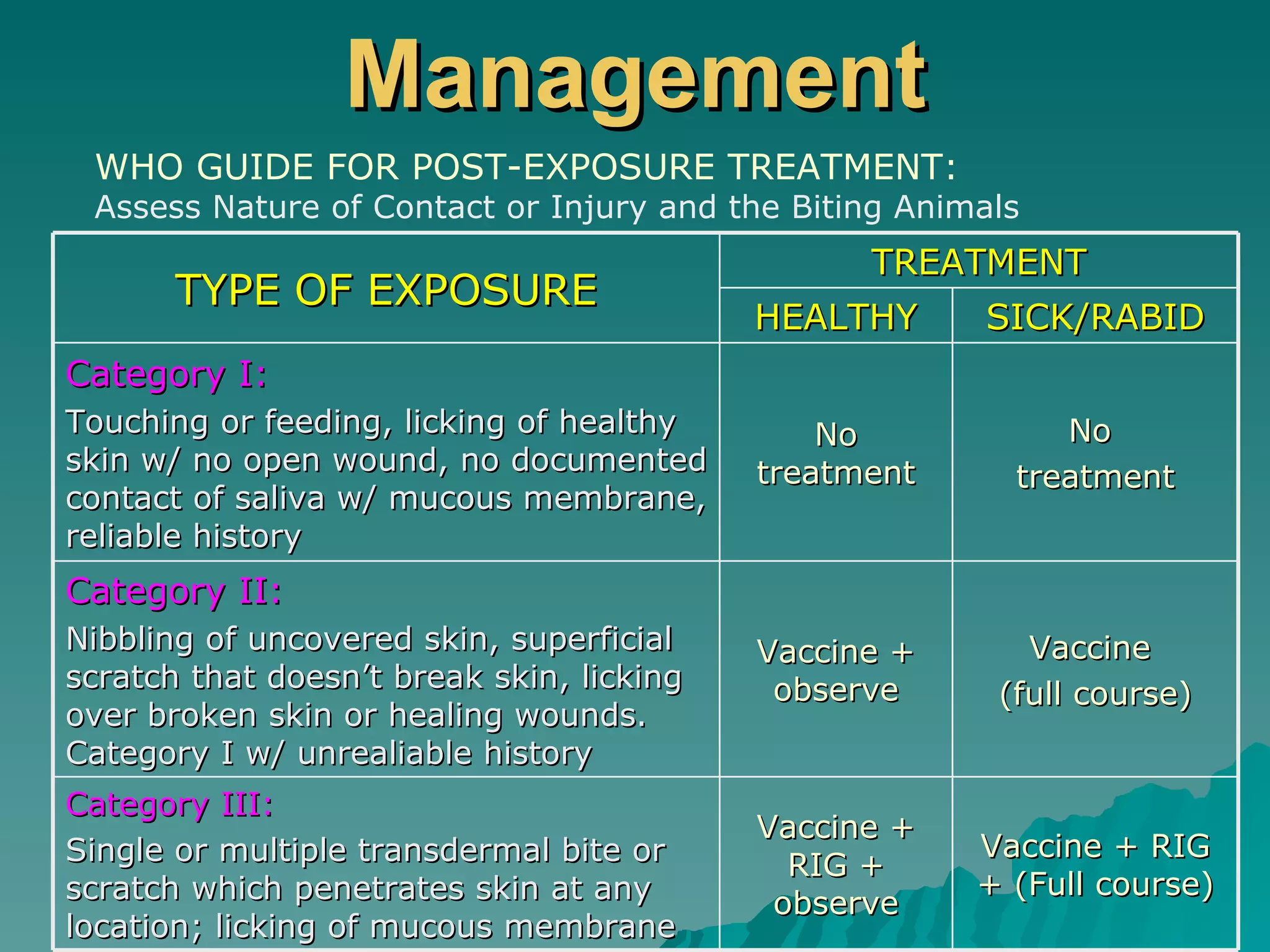
This document summarizes information about animal and insect bites, including rabies, snake bites, and arthropod bites. It describes the epidemiology, transmission, clinical manifestations, diagnosis, and management of rabies. It also discusses the toxicology, clinical manifestations, laboratory examination, and hospital and field management of snake bites. Finally, it provides information on hymenoptera (bee) bites, black widow spider bites, including their venom effects, manifestations, and treatment approaches.