Downloaded 78 times
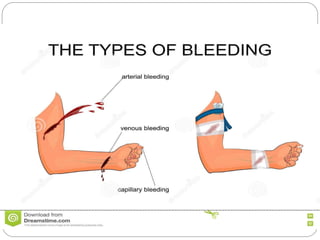
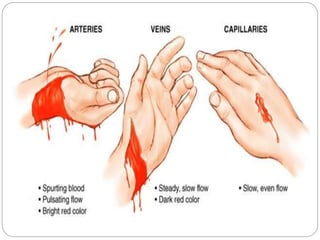
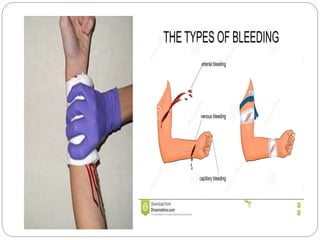

1. Hemorrhage is defined as the escape of blood from blood vessels. It can be classified based on the type of vessel (arterial, venous, capillary), timing (primary, reactionary, secondary), visibility (revealed, concealed), duration (acute, chronic), and type of intervention (surgical, non-surgical). 2. Clinical features depend on the amount and speed of blood loss, and can include increasing pallor, pulse, restlessness, signs of shock like cold skin and reduced urine output. Acute blood loss is monitored through pulse, blood pressure, and urine output. 3. Control techniques include direct pressure, elevation, tourniquets, cauterization















































































