Management of Dog bite and associated complications .ppt
4.
Rabies isan invariably lethal, acute viral dx of
the CNS that affect all mammals usually
transmitted by infected secretions.
Transmission of rabies to humans takes place
thro’ exposure to saliva during a bite by an
infected animal.
An effective rabies vaccine was first developed
over a century ago, making rabies a
preventable disease.
5.
Dogs arecommonly used for security and as
pets by most people in Nigeria, however it is
also used for hunting and occasionally serve as
source of protein.
Despite its usefulness, dogs can be very
harmful to humans when they are rabid.
6.
Rabies andrabies related viruses are in the
family Rabdoviridae with at least seven distinct
types, with genus lyssa-virus.
Isolates of rabies virus from different animals
species differ in their antigenic and biologic
property.
Rabies viruses are bullet-shaped, enveloped
single stranded RNA virus of negative polarity.
7.
An understandingof epizootiology of rabies is necc
in evaluating the risk of exposure and need for
rabies PEP in humans.
Rabies is fd in mammals in all regions of the world
with possible exception of Antarctica.
Rabies exist in two forms:
Urban (furious) rabies, propagated chiefly by un
immunized domestic dogs.
Sylvatic (dumb) rabies, propagated by skunks,
raccoons, mongoose, foxes and bat.
8.
World wideincidence of rabies is estimated at
more then 30,000 cases per year.
Southeast Asia, the Philippines, Africa and
Indian subcontinents are areas where the dx is
especially common.
The main reservoir of rabies world wide is
domestic dogs.
9.
Increased travelof human, along with
intentional and unintentional translocation of
animals has made the recognition of clinical
rabies and its prevention of increasing
importance.
In a 12-yr retrospective study (UBTH):
143 cases of dog bite
1 victim of rabies.
10.
A decade ofexperience in two hosp in Sokoto:
16 cases of rabies.
Over 900 victims of dog bite.
A 10 year experience in ABUTH Zaria:
A single case of rabies
81 cases of dog bite
Rabies in insectivorous bat occur in UK, Europe, USA,
Canada and Africa, essentially every locality where
bats are found.
11.
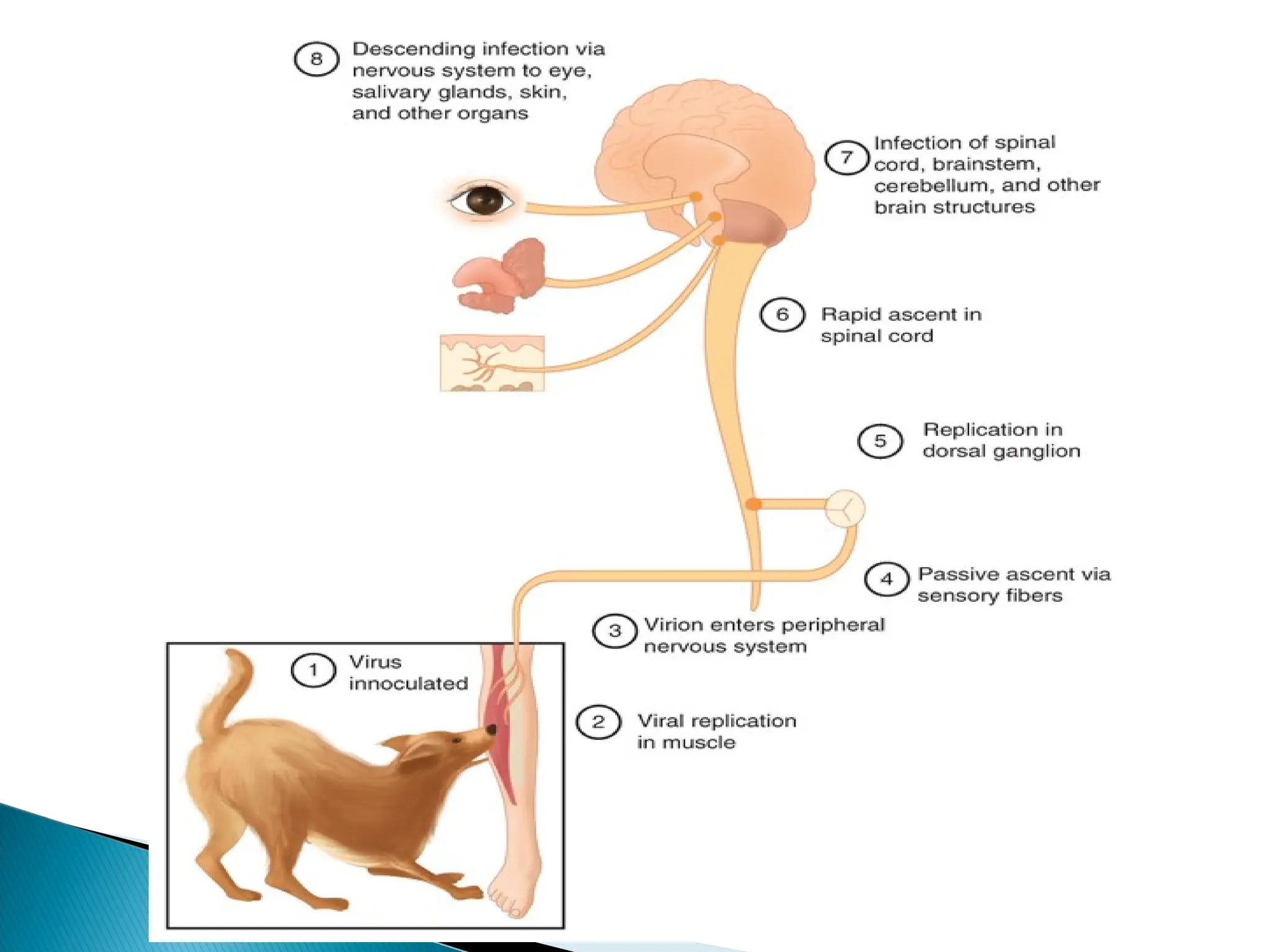
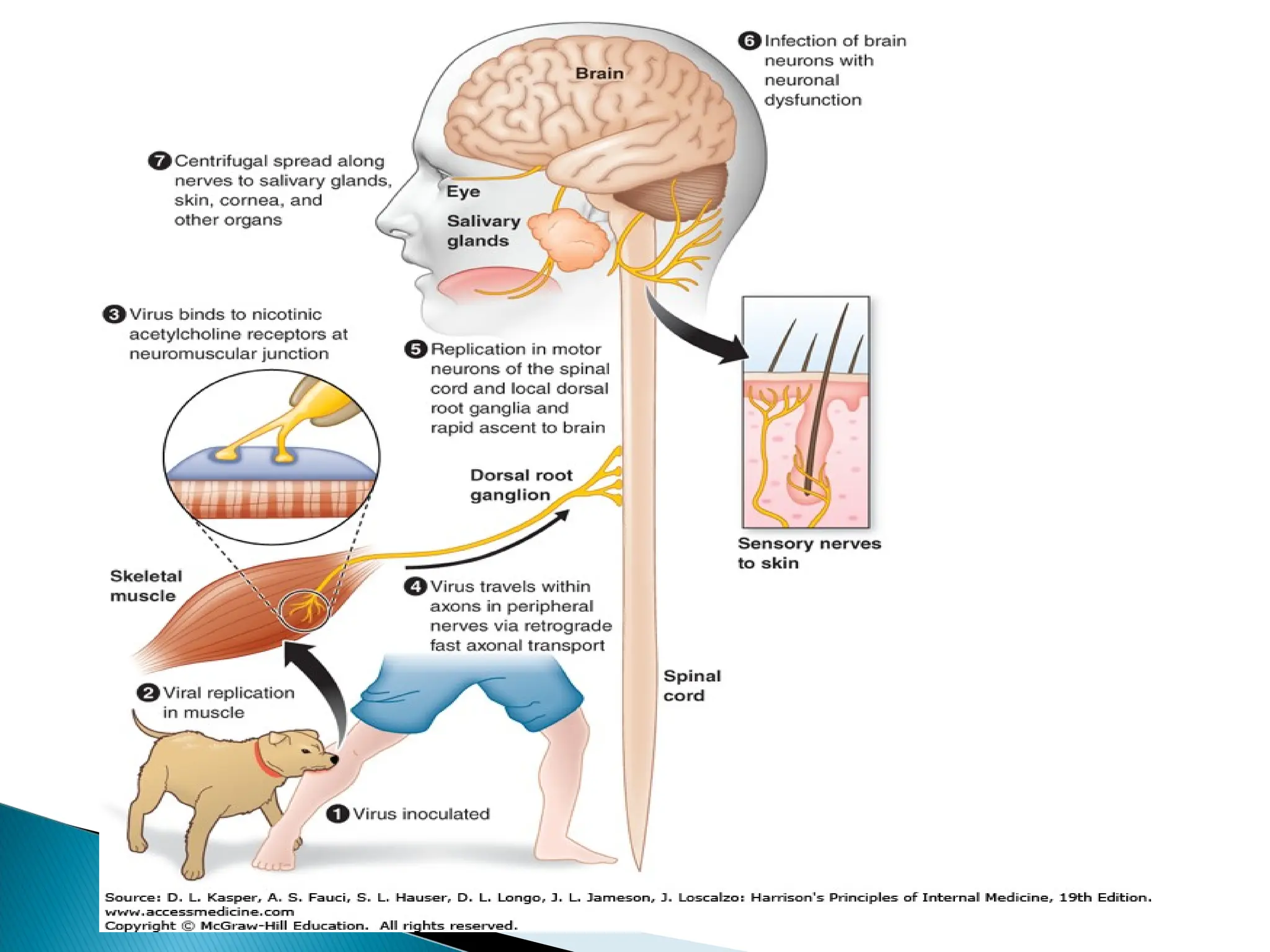
The firstevent in rabies is the inoculation of the
virus through the skin, usually through a bite that
delivers virus laden-saliva.
Initial viral replication appear to occur within the
striated muscle cell at the site of inoculation
.
Peripheral nervous system is thus exposed.
virus then spread centripetally CNS at rate of
→
3mm/hr.
14.
Virus oncein the CNS replicates almost exclusively
in the gray matter.
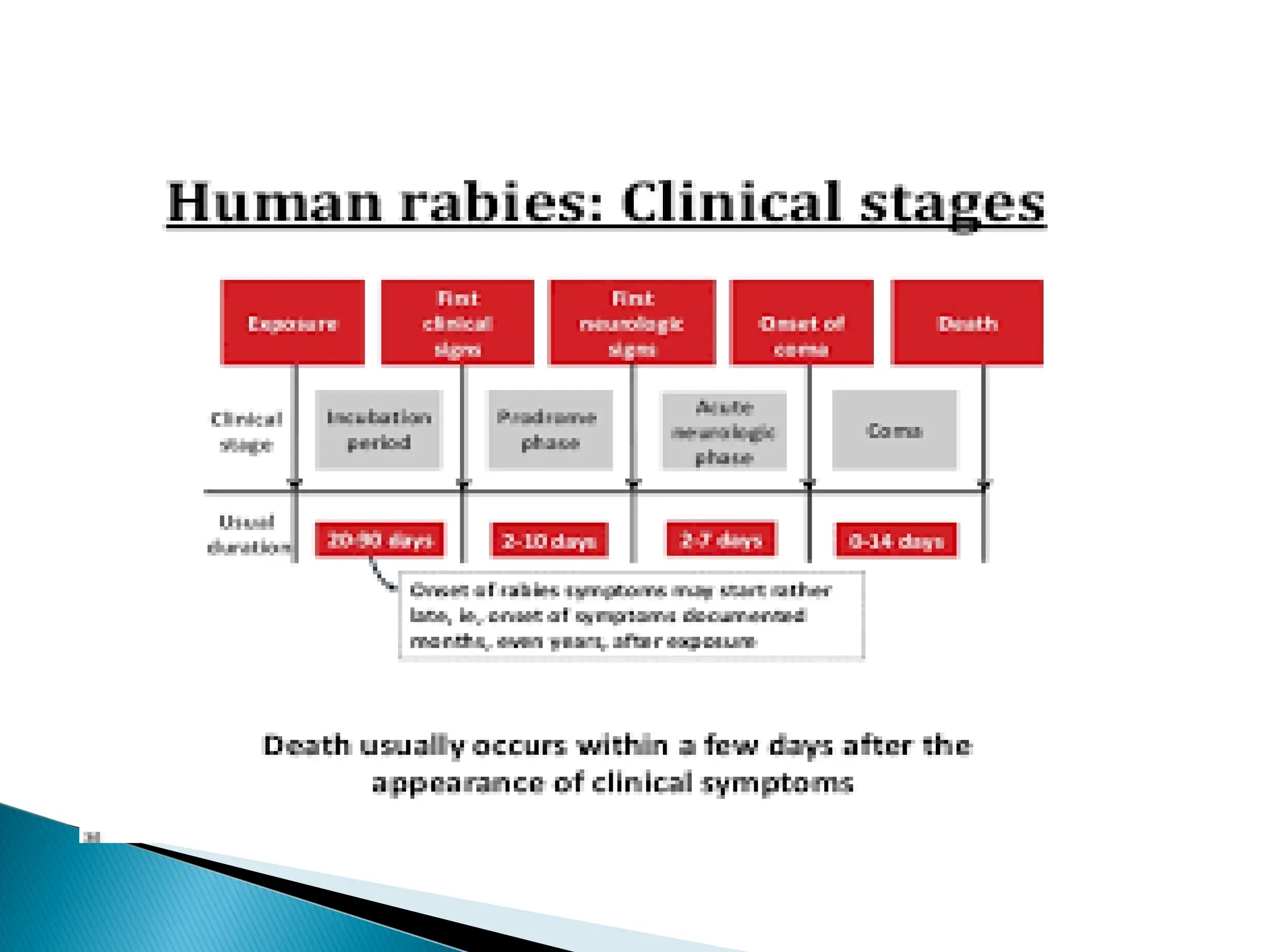
Incubation period of rabies is exceedingly variable
ranging from 7 days to >1 year (mean 1 to
2months) and apparently dependent on :
amount of virus introduced
Amount of tissue involved
Actual distance that the virus has to travel from site
of inoculation to the CNS.
16.
Rate of infectionand mortality are:
Highest from bite on the face
Intermediate from bite on the hand and arm
Lowest from bite on the leg.
Cases of human rabies with extended incubation
period (2 to 7 years) have been reported but
they are rare.
17.
The mostcharacteristic pathologic finding of
rabies in the CNS is the formation of
cytoplasmic inclusion
Negri bodies.
Negri bodies are absent in 20% of cases.
19.
Clinical manifestation ofrabies can be divided
into four stages:
1. Non specific prodrome
2. Acute encephalitic phase
3. Profound dysfunction of brainstem centre
4. Death or in rare cases recovery
20.
Rabies mayalso present as an ascending
paralysis resembling the Laundry/Guillain
Barre syndrome.
Paralytic rabies also occur in southeast Asia
among person with canine exposure.
21.
Non specific, CBC, mild CSF pleocytosis.
Rabies virus specific antibodies in serum and
CSF:
Indirect fluorescent antibody test.
Rapid fluorescent focus inhibition test
Reverse-transcriptase PCR on fresh saliva.
RT-PCR on skin biopsy sample.
22.
There isno specific treatment for clinical
rabies.
Death is virtually inevitable once clinical signs
develop.
Medical management is supportive and
palliative
24.
Bites andscratches from a potentially rabid animal
should be thoroughly washed with soap and water.
After all soap has been removed, cleanse with
benzyl ammonium hydrochloride (Zephiram)
Wound that have broken the skin should receive
tetanus prophylaxis.
Bite by a seemingly healthy animal requires
surveillance.
25.
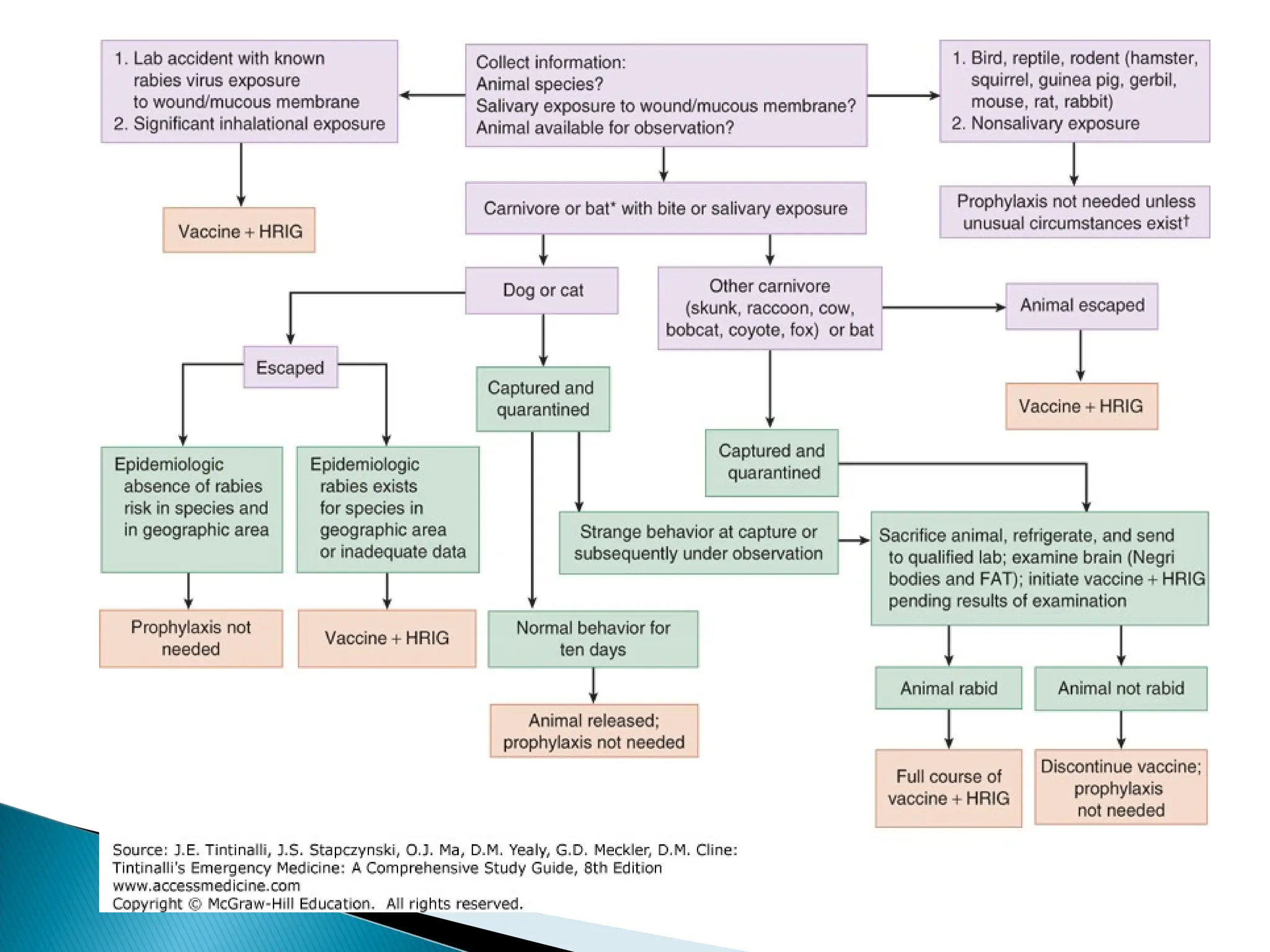
PEP shouldbe given in cases of rabid or
suspected rabid bite or the status of
immunization is not known.
Human rabies immune globulin (HRIG) is
injected at a dose of 20Units/kg of body wt.
Human diploid cell vaccine (1ml) should given
on days 0 , 3, 7, 14 and 28.
26.
Is availableto persons at the risk of rabies
exposure.
The recommendation is that a series of 1ml
doses of modern cell culture vaccine
administered intramuscularly on days 0, 7 and
21or 28.
If an exposure occurs, a previously immunized
person should receive post exposure boosters
consisting of two doses on 3 days apart.