Downloaded 85 times
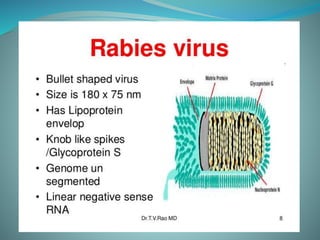
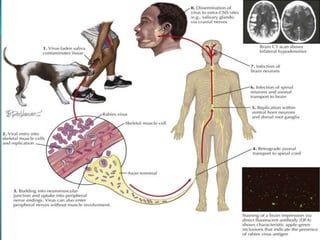





Rabies is a viral disease causing acute encephalitis in warm-blooded animals, primarily transmitted to humans through bites or scratches from infected animals, mostly dogs. Symptoms include bizarre behavior, hydrophobia, and paralysis, with a high fatality rate once they develop, necessitating immediate treatment including wound care and vaccinations. Prevention involves pre-exposure and post-exposure prophylaxis, with attention to timely management and infection control in cases of confirmed rabies.


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
