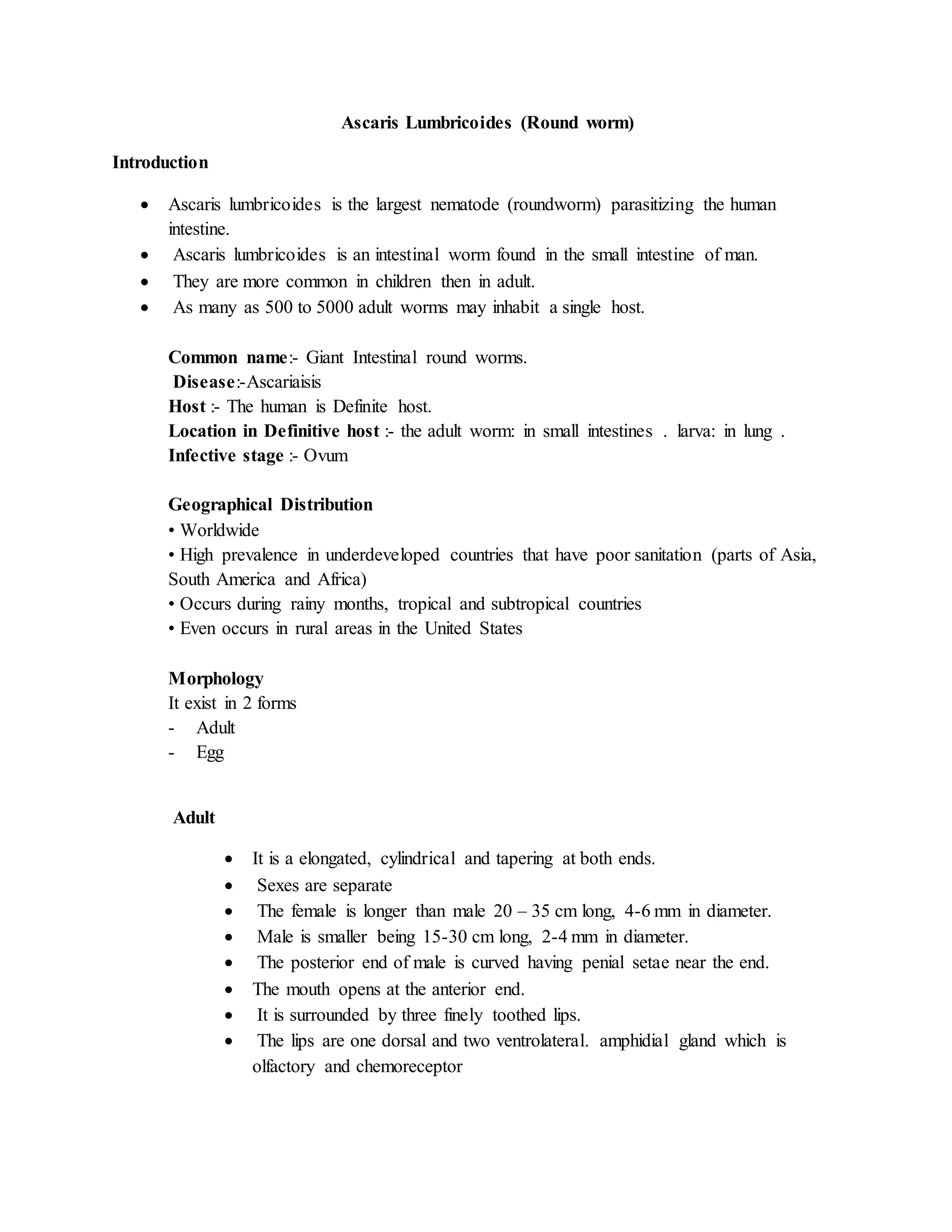
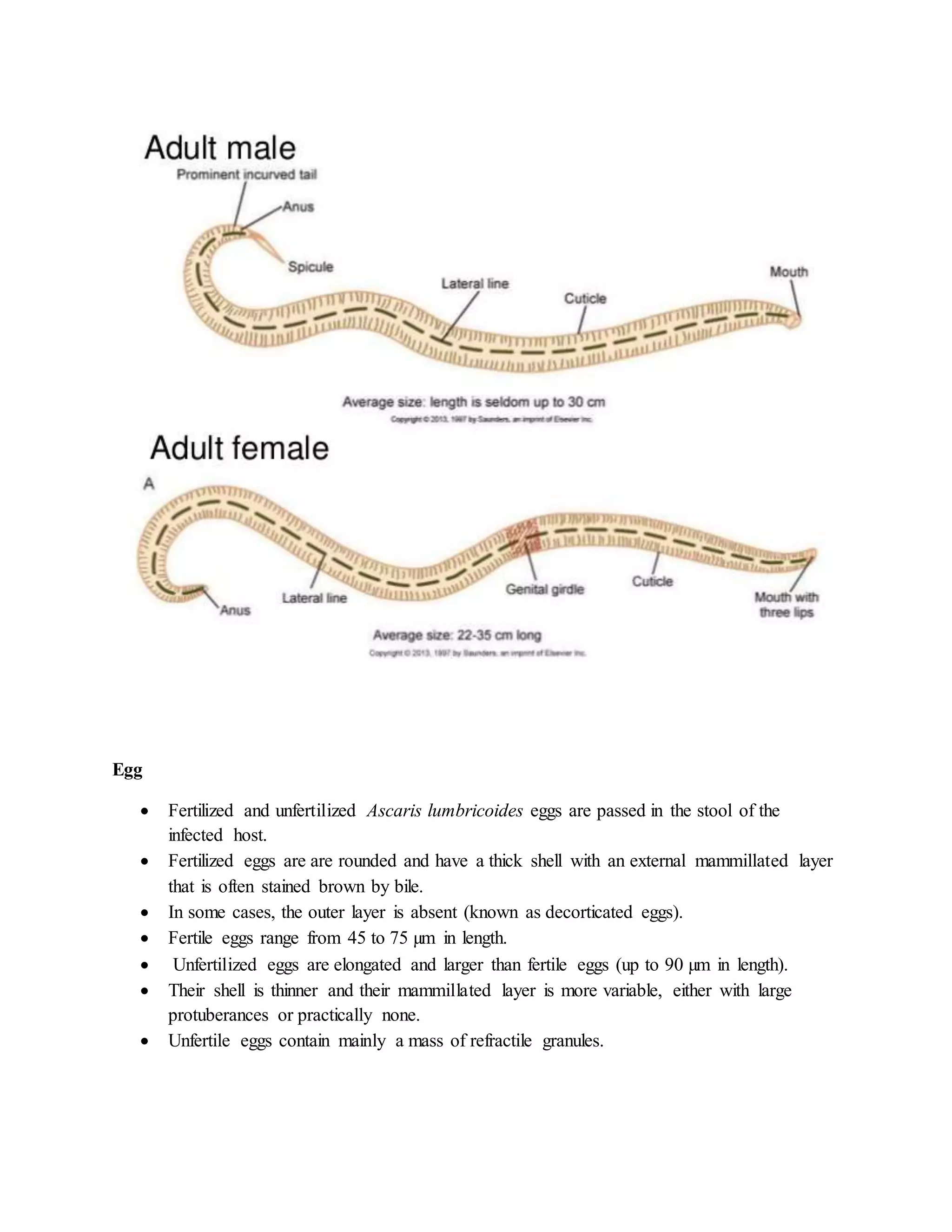
Ascaris lumbricoides, also known as the giant intestinal roundworm, is a parasitic nematode that infects the small intestine of humans. It has a worldwide distribution, especially in tropical and subtropical areas with poor sanitation. The adult worms can reach lengths of 20-35 cm in females and 15-30 cm in males. The life cycle involves fertilized eggs passing in feces and developing into infective larvae outside the body. People become infected by ingesting these embryonated eggs. The larvae hatch in the intestine, penetrate the intestinal wall, migrate through the lungs, are swallowed and pass into the intestine where they mature into adult worms. Most infections are asymptomatic, but symptoms can include abdominal pain,