Downloaded 121 times
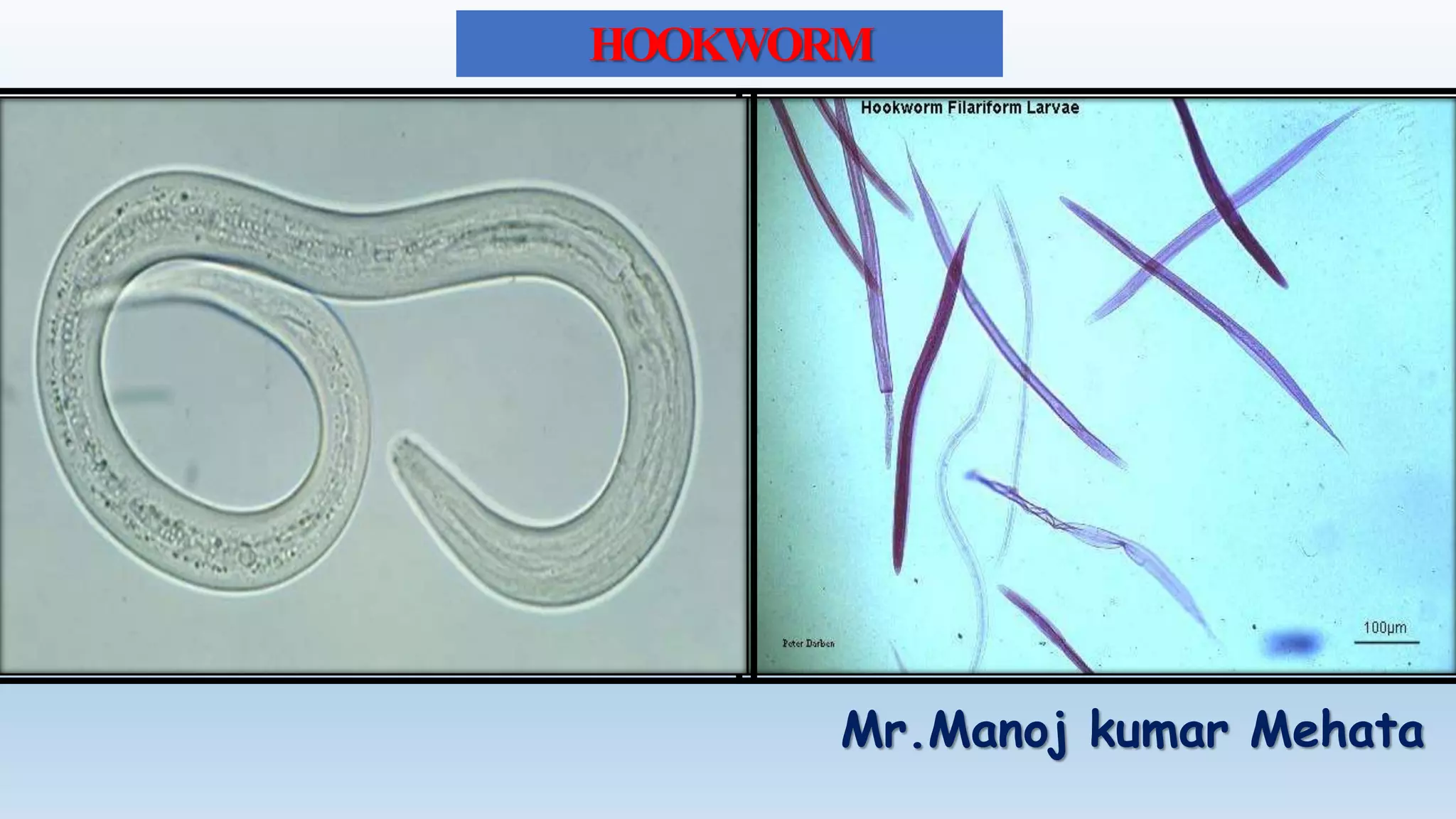


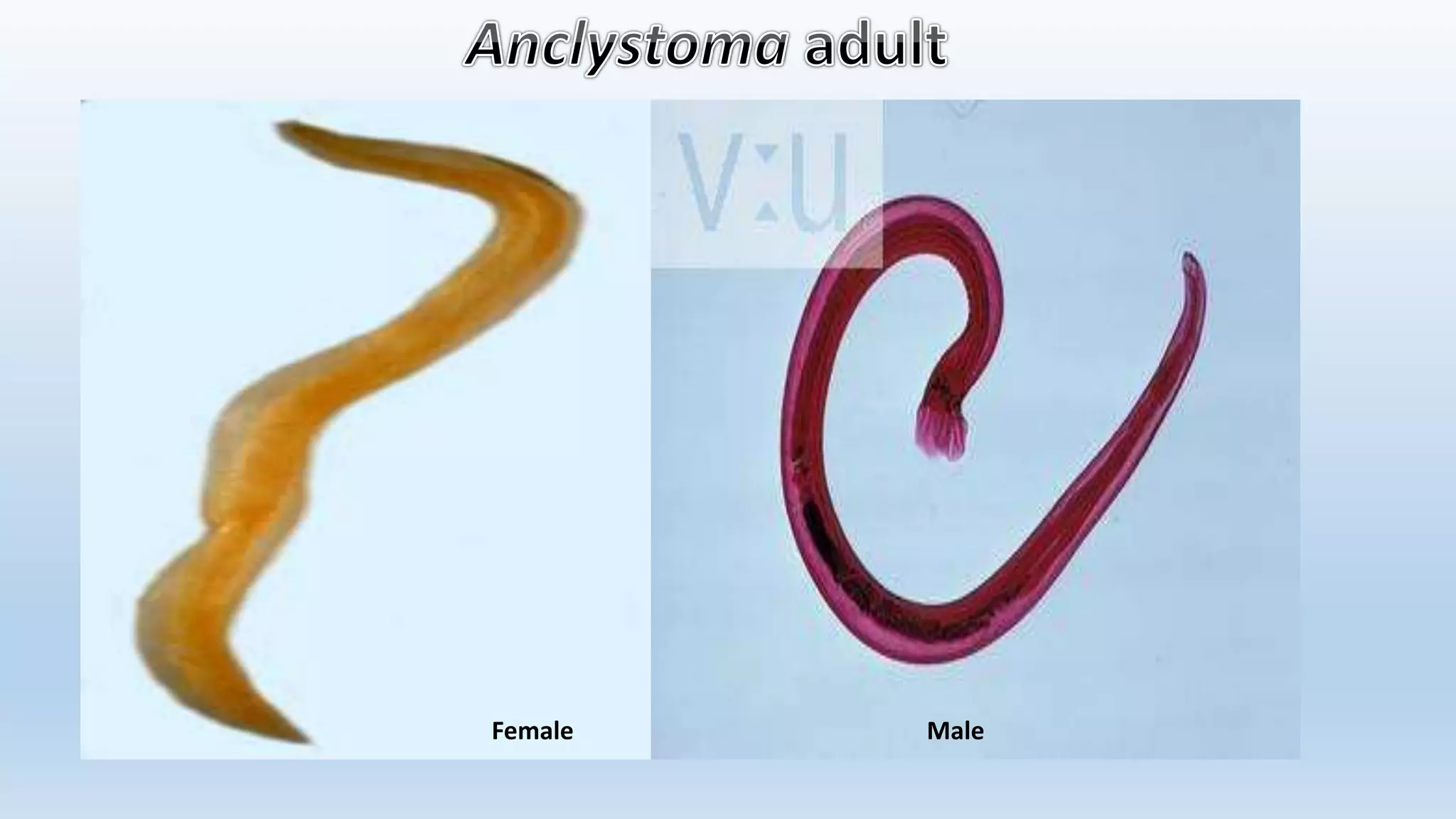
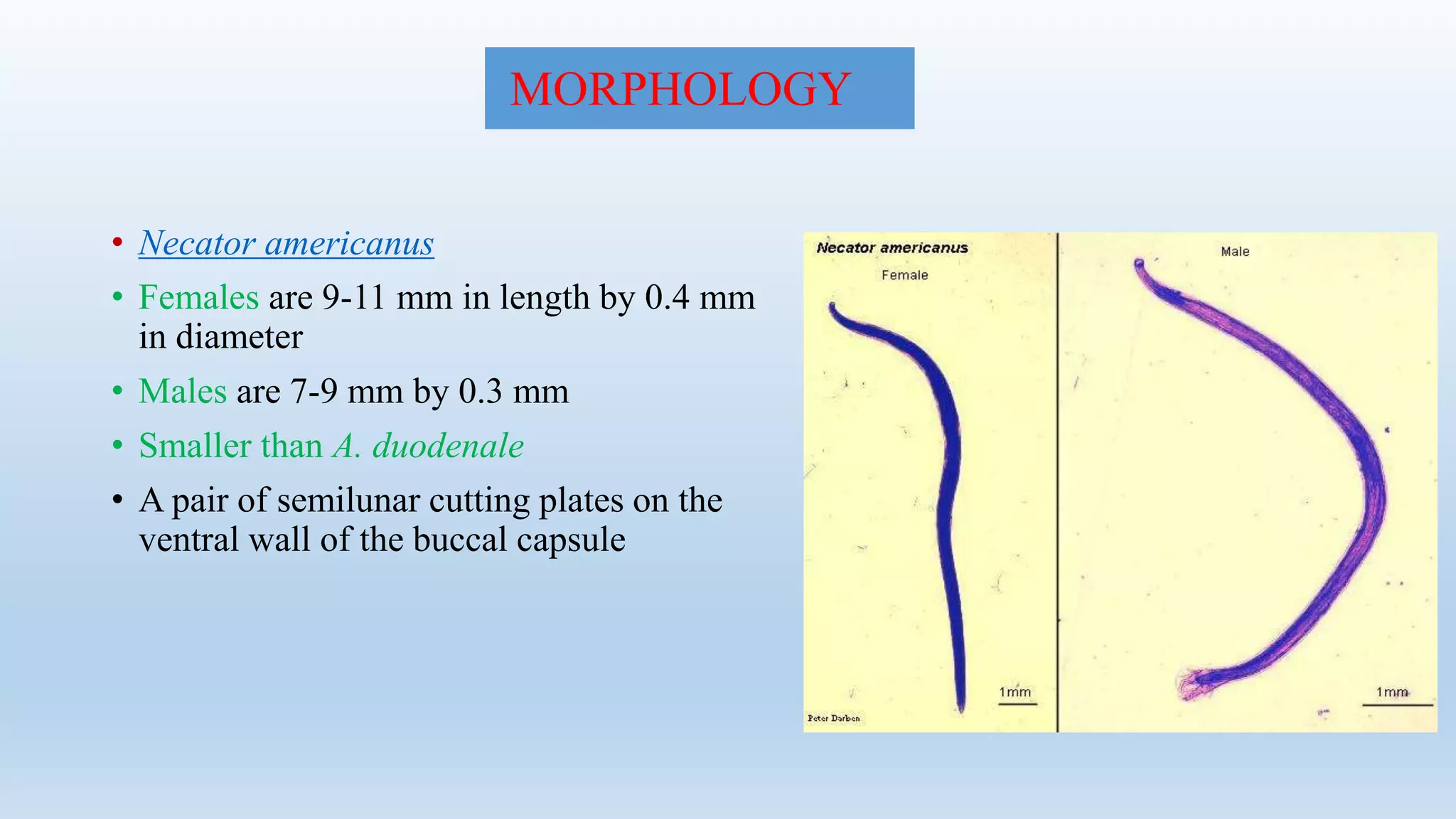

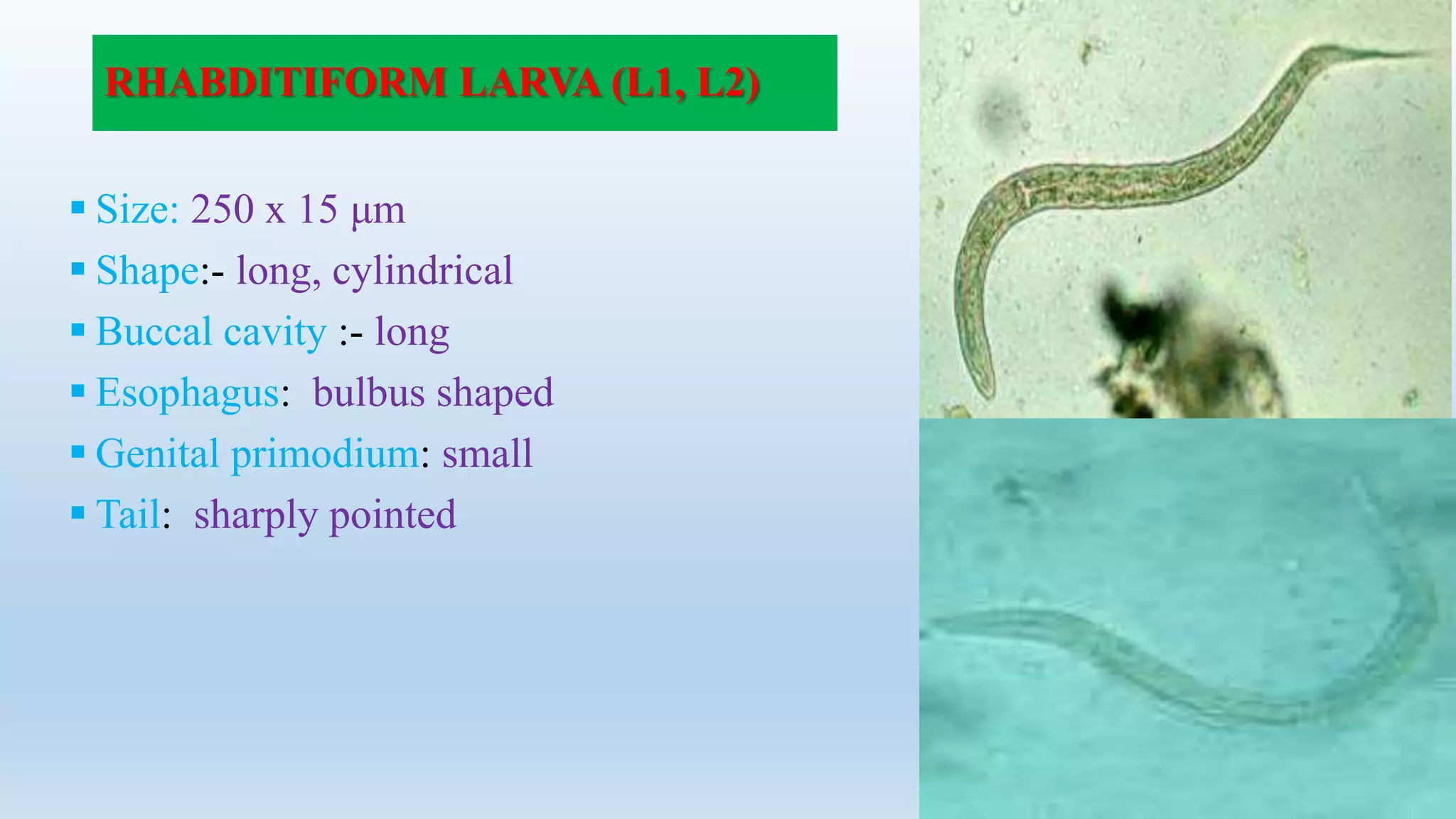


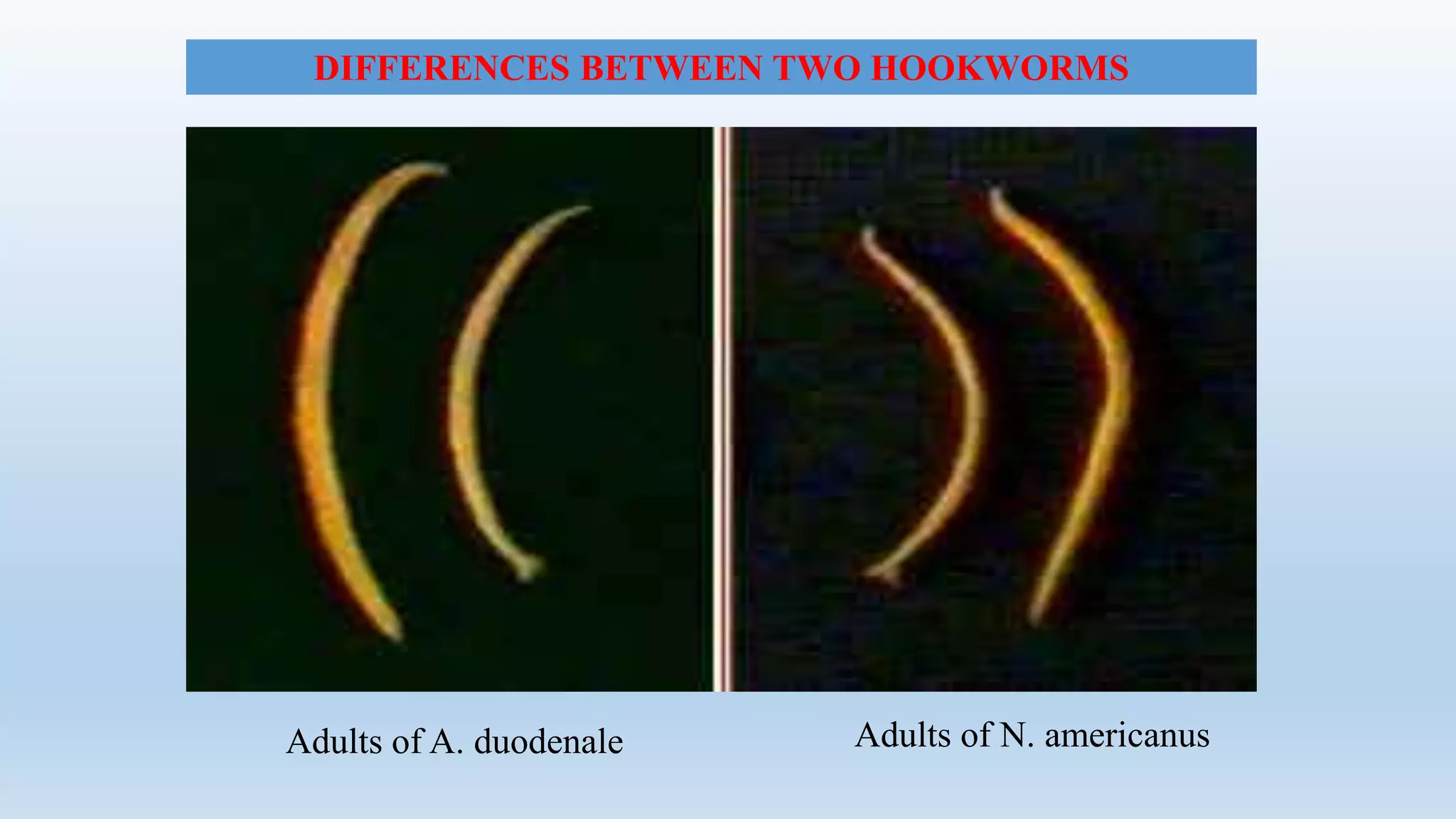



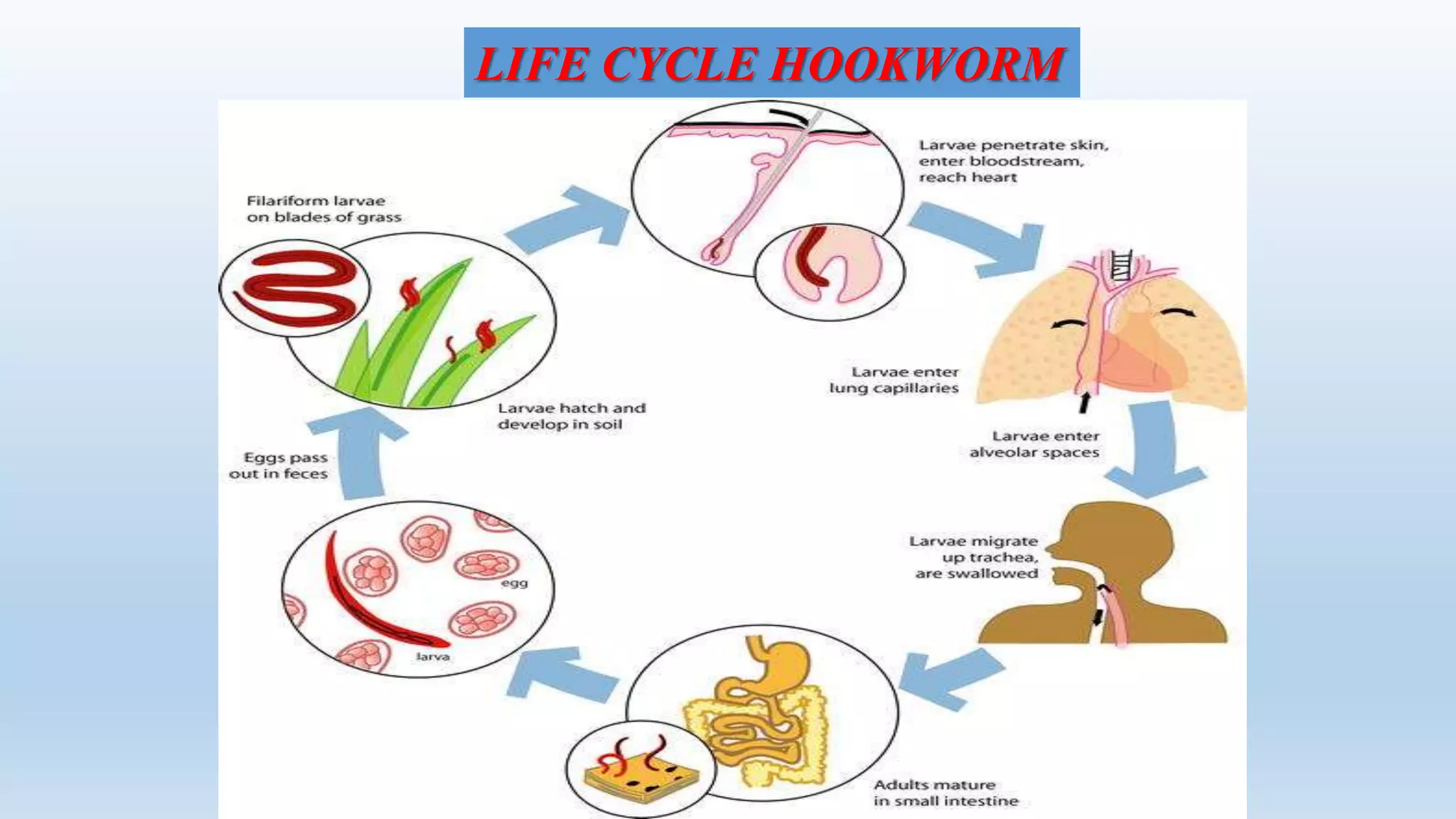






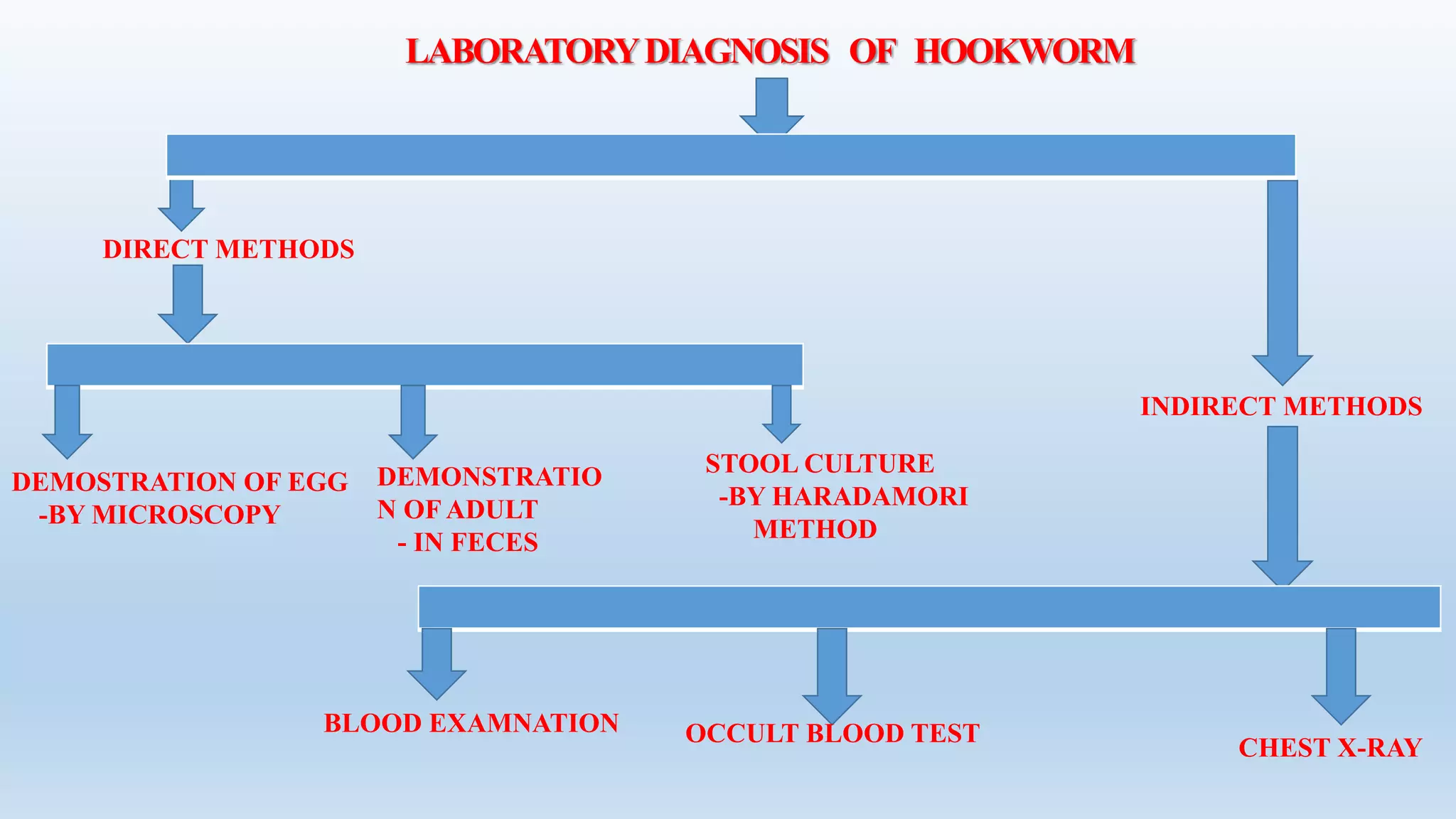


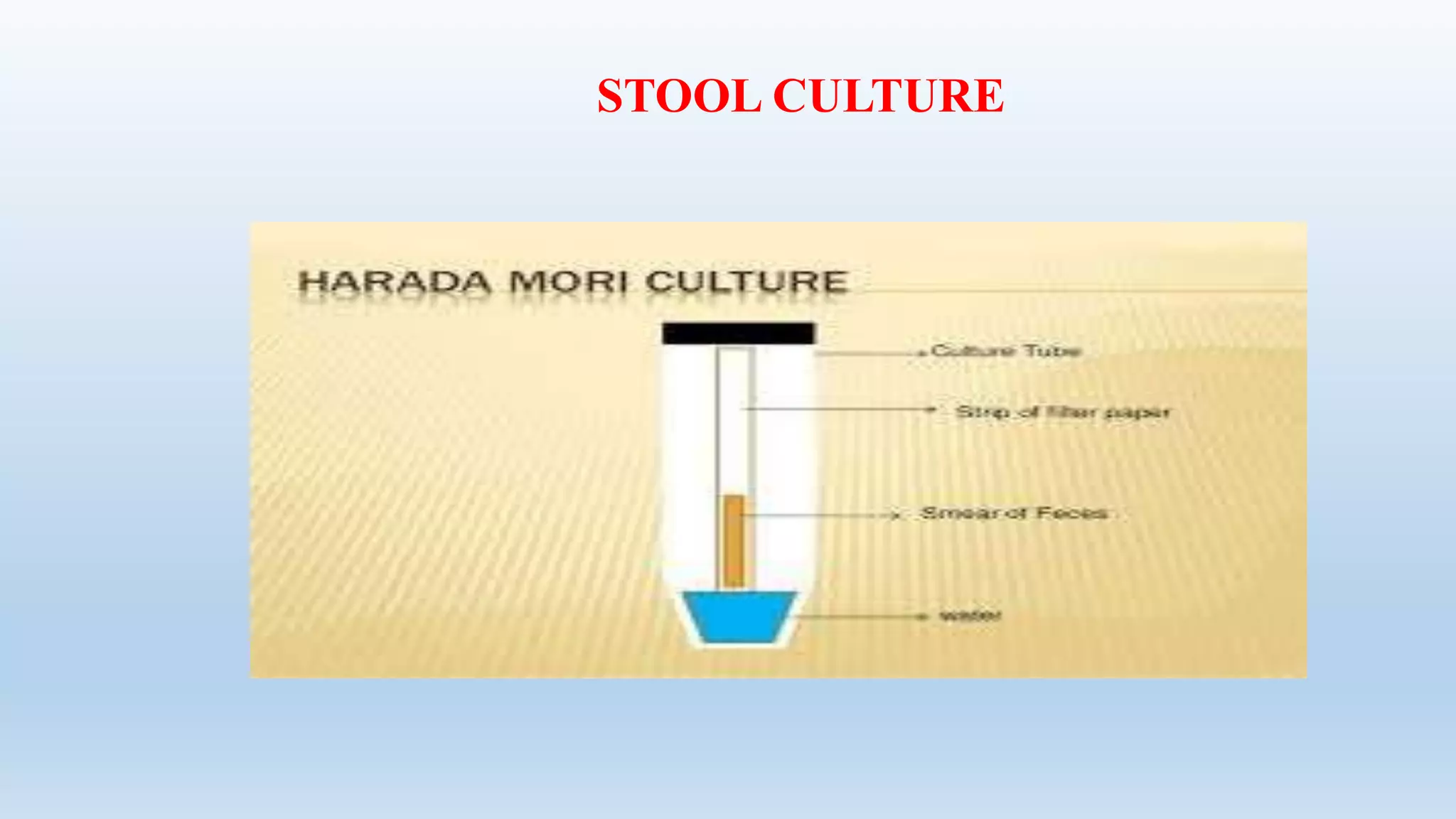


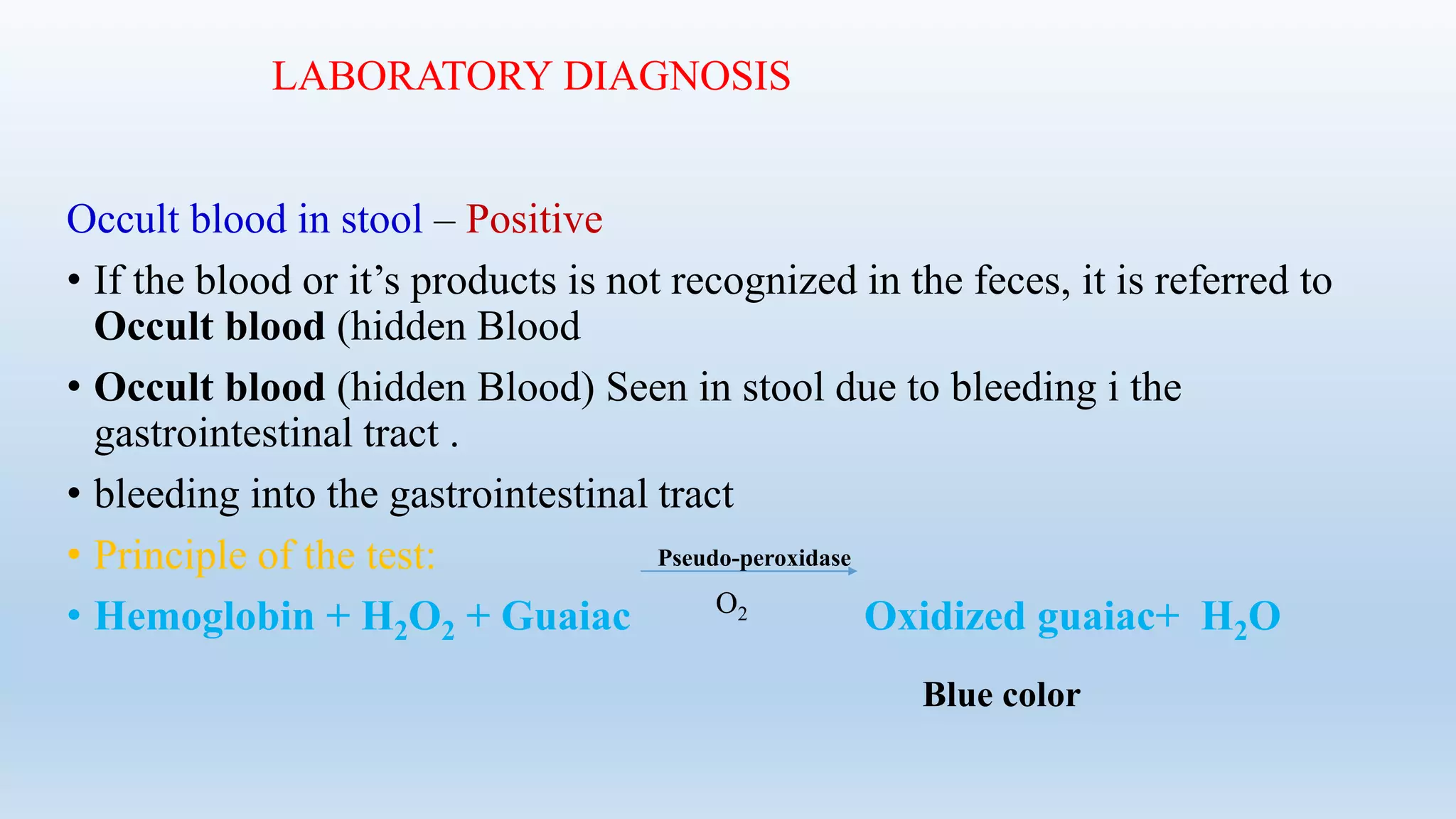

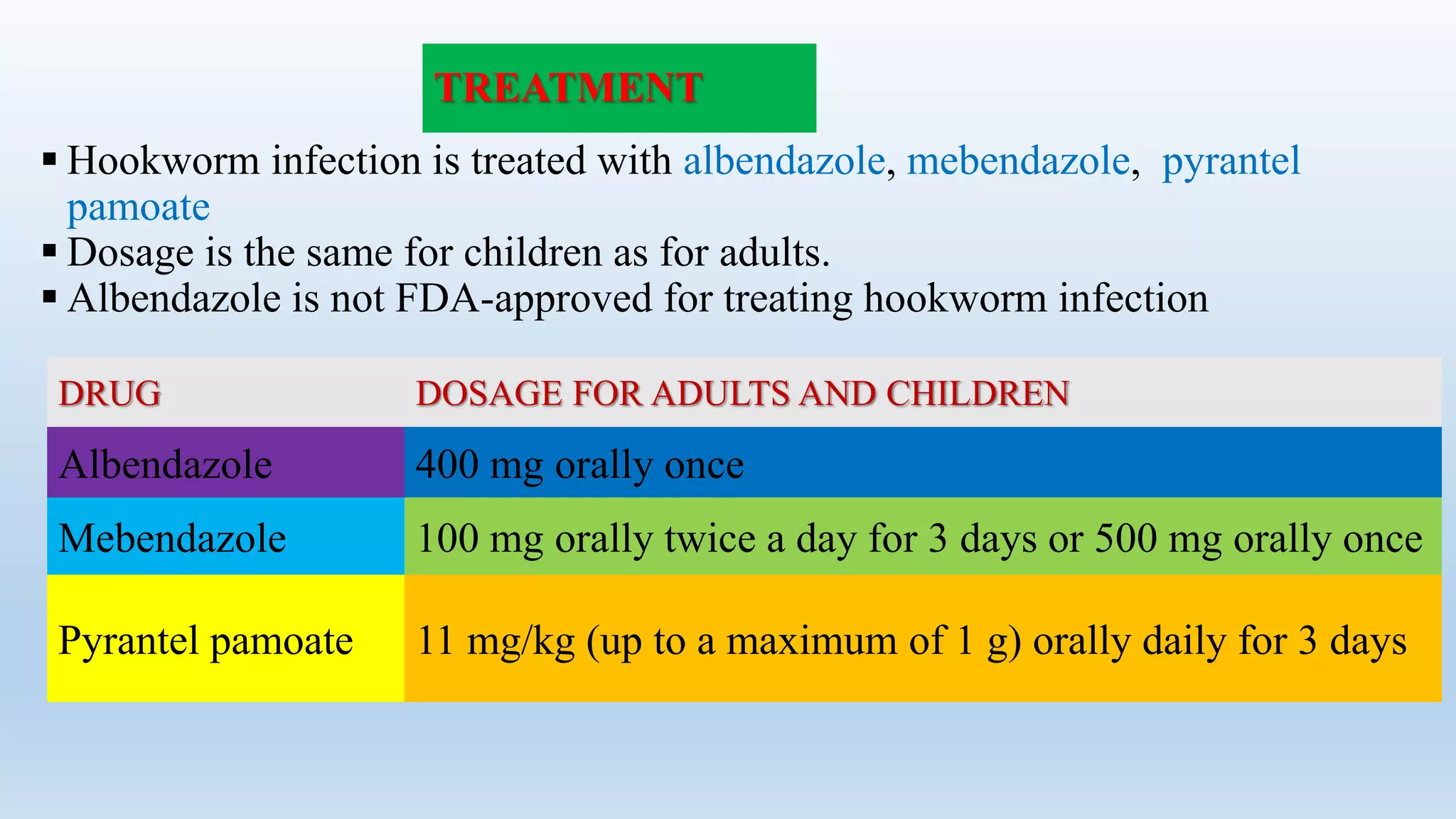


This document provides information on hookworm, including its taxonomic classification, epidemiology, introduction, morphology, life cycle, modes of transmission, signs and symptoms, pathogencity, clinical diagnosis, laboratory diagnosis, prevention, control, and treatment. It discusses two main species of hookworm that infect humans - Ancylostoma duodenale and Necator americanus. Key details include that hookworm affects approximately 900 million people worldwide, living primarily in tropical and subtropical regions, and signs of infection include skin irritation, coughing, anemia, and iron deficiency.























































































