Downloaded 55 times




![Analgeia ctd…
Larynx/ cords/ trachea
- nebulization
- placement of local anaesthetic( LA) soaked pellets in pyriform fossa
-Spraying LA through a 16 G epidural catheter via working channel of the
fiberoptic laryngoscope[ spray as you go technique]
-Local blocks
Superior laryngeal branch – inferior to greater cornu of hyoid
Recurrent laryngeal branch- translaryngeal throught cricothyroid membrane
using negative aspiration to air
-Ultrasound guidance- higher success rates](https://image.slidesharecdn.com/afoitiva-181118163117/75/AWAKE-FIBEROPTIC-INTUBATION-TIVA-simplified-7-2048.jpg)



![Pump failure during TIVA
- Switching to conventional inhalational agents[ anticipate exaggerated
haemodynamic response]
-Restarting infusion manually with last flow rates[ ml/hr]
-Restarting TIVA from the beginning](https://image.slidesharecdn.com/afoitiva-181118163117/75/AWAKE-FIBEROPTIC-INTUBATION-TIVA-simplified-17-2048.jpg)

![Problems
-Accidental awareness- mainly due to inadequate knowledge of the operator/
equipment malfunction
[ Association of Anaesthetists of Great Britain and Ireland (AAGBI) and the Society for Intravenous Anaesthesia (SIVA)
Total Intravenous Anaesthesia 2017: guidelines for safe practice]
-Post operative apnoea
-Hyperalgesia
-Morbid obesity
-Propofol related infusion syndrome( uncommon)](https://image.slidesharecdn.com/afoitiva-181118163117/75/AWAKE-FIBEROPTIC-INTUBATION-TIVA-simplified-19-2048.jpg)


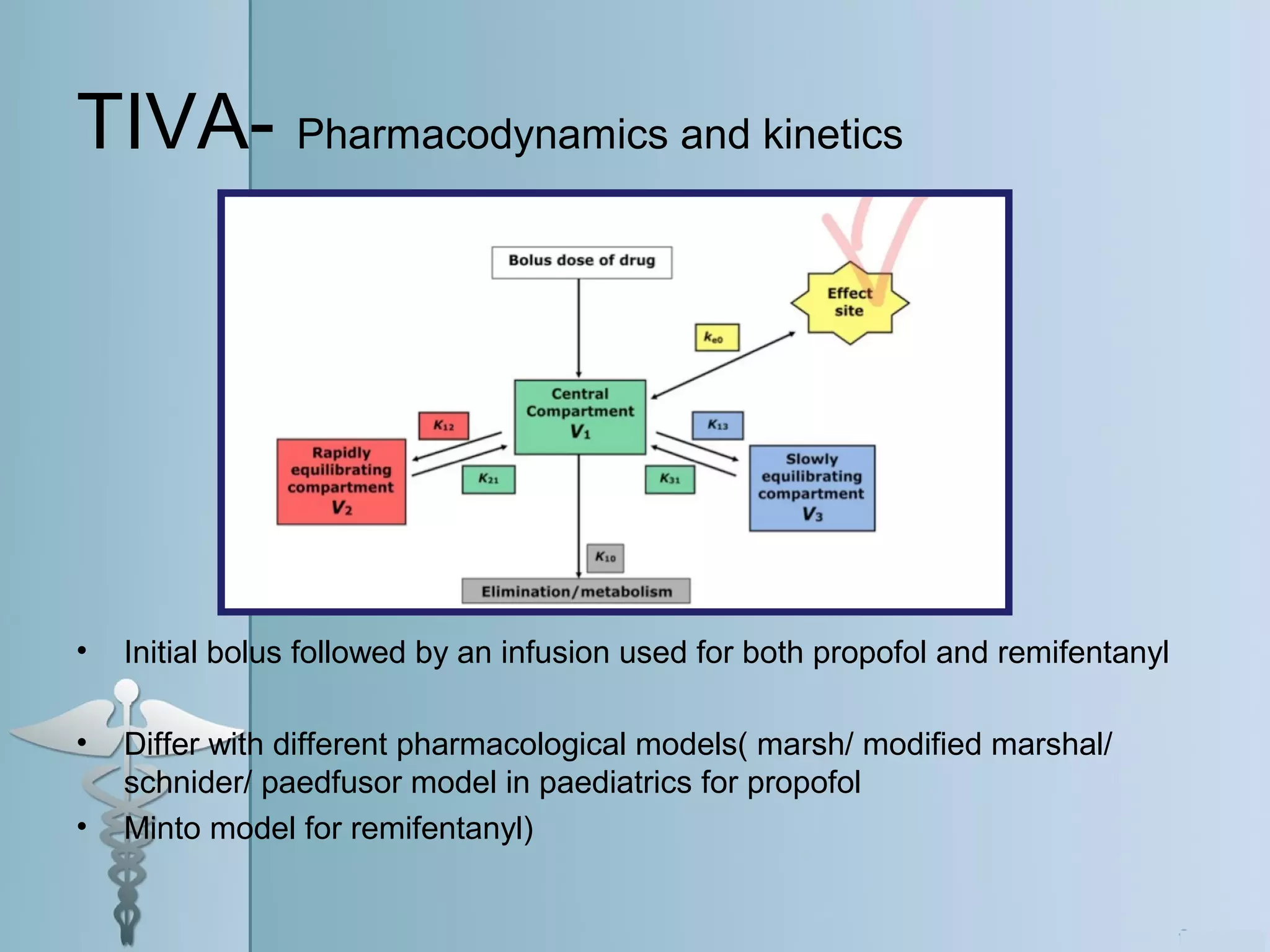
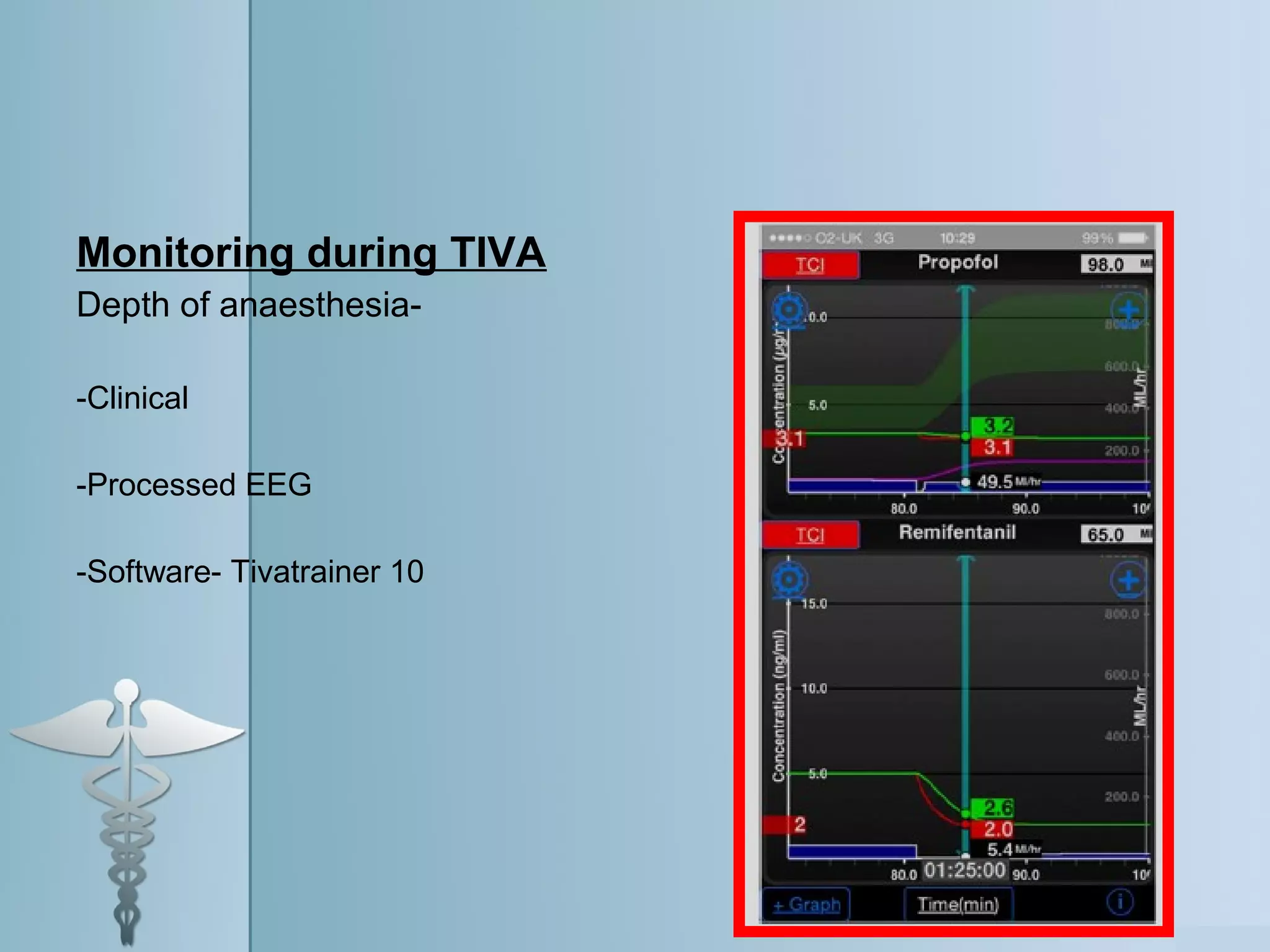
Awake fiberoptic intubation and total intravenous anesthesia (TIVA) are described. Awake fiberoptic intubation is the gold standard for predicted or known difficult airways and involves conscious sedation and analgesia during intubation. TIVA involves using intravenous propofol and remifentanyl infusions without inhalational gases. It has advantages like reduced postoperative nausea but risks include accidental awareness and postoperative apnea. Both techniques require monitoring and experience to perform safely.