Downloaded 67 times
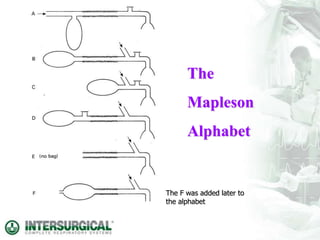
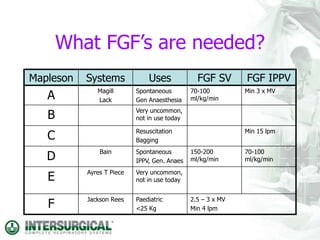
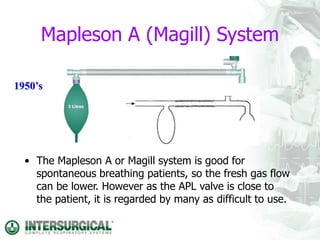
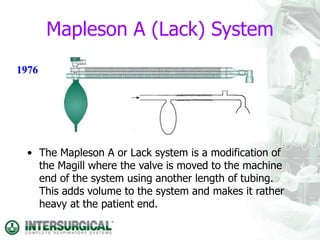


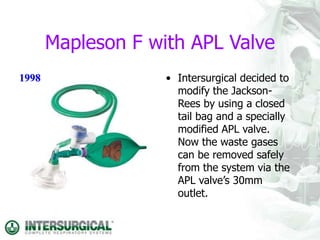
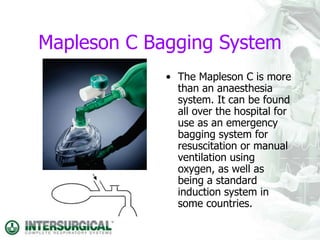

This document discusses different types of breathing systems used in anaesthesia. It describes the components and ideal properties of breathing systems. Open, semi-open, and semi-closed systems are defined. Several specific semi-open systems are outlined, including the Mapleson A, D, F systems. Semi-closed systems require CO2 absorbents and lower fresh gas flows than open systems. Types of semi-closed systems are also defined. The document emphasizes the importance of ensuring tight connections between breathing system components.











































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











