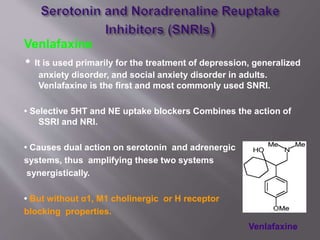
This document discusses depression, including its causes, symptoms, diagnosis and treatment options. It describes two main types of depression - exogenous depression, which usually follows traumatic life events, and endogenous depression, which is not associated with precipitating events and may be due to biochemical changes. Common symptoms of depression are then listed. The document goes on to discuss various treatment approaches for depression, including psychotherapy, electroconvulsive therapy, and several classes of antidepressant medications like SSRIs, SNRIs, TCAs, MAOIs and others. Side effects and mechanisms of action are provided for some of the antidepressant classes.






























![Depression [2002]](https://cdn.slidesharecdn.com/ss_thumbnails/depression-170814010933-thumbnail.jpg?width=640&height=640&fit=bounds)















![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)










































