Downloaded 18 times
![What Is In An ABG?
pH [H+
]
PCO2 Partial Pressure CO2
PO2 Partial Pressure O2
HCO3 Bicarbonate
BE Base Excess
SaO2 Oxygen Saturation](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-4-320.jpg)





















![PaO2
• Depends on FiO2.(usually 4-5 times)
• Depends on the barometric pressure and age
• PaO2age adjusted = 102- (age in yrs/3)
• Calculate PAO2- PaO2
• PAO2
normal A–a gradient is less than [age in years]/4 + 4
For every decade a person has lived, their A–a gradient is
expected to increase by 1 mmHg](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-27-320.jpg)
![Are the data consistent?
• The Henderson Equation:
[ ] −
+
×=
3
2
24
HCO
PaCO
H](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-28-320.jpg)
![Convert pH to [H+
] :
• Subtract the last two digits of a pH from 80
example: calculated [H+
] of 24
pH of (80-56)~7.56
example: calculated [H+
] of 53
pH of (80-27)~7.27](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-29-320.jpg)
![Relationship between [H+
] & pH](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-30-320.jpg)

![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis ↓ ↓
Metabolic Alkalosis
Acute Respiratory Acidosis
Chronic Respiratory Acidosis
Acute Respiratory Alkalosis
Chronic Respiratory Alkalosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-32-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis ↓ ↓ ↓
Metabolic Alkalosis
Acute Respiratory Acidosis
Chronic Respiratory Acidosis
Acute Respiratory Alkalosis
Chronic Respiratory Alkalosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-33-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis
Metabolic Alkalosis ↑ ↑
Acute Respiratory Acidosis
Chronic Respiratory Acidosis
Acute Respiratory Alkalosis
Chronic Respiratory Alkalosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-34-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis
Metabolic Alkalosis ↑ ↑ ↑
Acute Respiratory Acidosis
Chronic Respiratory Acidosis
Acute Respiratory Alkalosis
Chronic Respiratory Alkalosis
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis
Metabolic Alkalosis ↑ ↑ ↑
Acute Respiratory Acidosis
Chronic Respiratory Acidosis
Acute Respiratory Alkalosis
Chronic Respiratory Alkalosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-35-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis
Metabolic Alkalosis
Acute Respiratory Acidosis ↓ ↑
Chronic Respiratory Acidosis ↓ ↑
Acute Respiratory Alkalosis
Chronic Respiratory Alkalosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-36-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis
Metabolic Alkalosis
Acute Respiratory Acidosis ↓ ↑ ↑
Chronic Respiratory Acidosis ↓ ↑ ↑↑
Acute Respiratory Alkalosis
Chronic Respiratory Alkalosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-37-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis
Metabolic Alkalosis
Acute Respiratory Acidosis
Chronic Respiratory Acidosis
Acute Respiratory Alkalosis ↑ ↓
Chronic Respiratory Alkalosis ↑ ↓](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-38-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis
Metabolic Alkalosis
Acute Respiratory Acidosis
Chronic Respiratory Acidosis
Acute Respiratory Alkalosis ↑ ↓ ↓
Chronic Respiratory Alkalosis ↑ ↓ ↓↓](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-39-320.jpg)
![Simple Acid-Base Disorders:
Type of Disorder pH PaCO2 [HCO3]
Metabolic Acidosis ↓ ↓ ↓
Metabolic Alkalosis ↑ ↑ ↑
Acute Respiratory Acidosis ↓ ↑ ↑
Chronic Respiratory Acidosis ↓ ↑ ↑↑
Acute Respiratory Alkalosis ↑ ↓ ↓
Chronic Respiratory Alkalosis ↑ ↓ ↓↓](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-40-320.jpg)

















![Rules of Compensation:
• Metabolic Acidosis
– PaCO2 should fall by 1 to 1.5 mm Hg x the fall in
plasma [HCO3]
– Winters formula
• PaCO2 = 1.5 x HCO3 + 8 (+/-2)
• Metabolic Alkalosis
– PaCO2 should rise by .5 to 1 mm Hg x the rise in
plasma [HCO3]
– Modified formula
• PaCO2 = 0.7 x HCO3 + 20](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-60-320.jpg)
![Rules of Compensation:
• Acute Respiratory Acidosis
– Plasma [HCO3] should rise by ~1mmole/l for
each 10 mm Hg increment in PaCO2
• Chronic Respiratory Acidosis
– Plasma [HCO3] should rise by ~4mmoles/l for
each 10 mm Hg increment in PaCO2](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-61-320.jpg)
![Rules of Compensation:
• Acute Respiratory Alkalosis
– Plasma [HCO3] should fall by ~2 mmole/l for
each 10 mm Hg decrement in PaCO2, usually
not to less than 18 mmoles/l
• Chronic Respiratory Alkalosis
– Plasma [HCO3] should fall by ~5 mmole/l for
each 10 mm Hg decrement in PaCO2, usually
not to less than 14 mmoles/l](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-62-320.jpg)







![Case #1:
• Steps 1&2: must know pH, PaCO2, HCO3
• pH=7.33, PaCO2=24, and HCO3=12
• Step 3: are the available data consistent?
[ ] −
+
×=
3
2
24
HCO
PaCO
H](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-70-320.jpg)
![Case #1:
• [H+]=48, equates to pH~7.32; data are thus
consistent
• What is the primary disorder?
• “_________Acidosis”
• Which variable (PaCO2, HCO3) is deranged
in a direction consistent with acidosis?
• Primary disorder is “Metabolic Acidosis”](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-71-320.jpg)




![Case #2: Steps 1, 2, and 3
• What baseline information is required?
• PaCO2=40 mm Hg, HCO3=7, pH=6.88
• Are the data internally consistent?
[ ] −
+
×=
3
2
24
HCO
PaCO
H](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-76-320.jpg)
![Case #2:
• [H+
]~140, which equates to a pH~6.85, so
data are internally consistent
• What is the primary disturbance?
• “___________ Acidosis”
• Which variable is deranged in a direction
which is consistent with acidosis?
• PaCO2 WNL, ergo, “Metabolic Acidosis”](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-77-320.jpg)
![Is compensation appropriate?
• Metabolic Acidosis
– PaCO2 should fall by 1 to 1.5 mm Hg x the fall
in plasma [HCO3]
• HCO3 decreased by 17, so we expect PaCO2
to be decreased by 17-26
• PaCO2 WNL; since PaCO2 inappropriately
high, there is a combined metabolic acidosis
and respiratory acidosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-78-320.jpg)


![Case #3:
• What baseline information is available?
• pH=7.55, PaCO2=66
• ‘lytes: Na+
=166, K+
=3.0, Cl-
=90, HCO3=56
• Are the data internally consistent?
[ ] −
+
×=
3
2
24
HCO
PaCO
H](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-81-320.jpg)
![Case #3:
• [H+]~28, equates to pH~7.55; consistent
• What is the primary abnormality?
• “_________ Alkalosis”
• PaCO2↑ed, HCO3 ↑ed, therefore…….
• “Metabolic Alkalosis” presumed due to
emesis
• Is compensation appropriate?](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-82-320.jpg)
![Case #3:
• Metabolic Alkalosis
– PaCO2 should rise by .5 to 1 mm Hg x the rise
in plasma [HCO3]
• HCO3 ↑ed by 32; PaCO2 should ↑ by 16-32
• PaCO2 ↑ed by 26, so compensation appears
appropriate
• What about multiple risk factors for lactic
acidosis?](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-83-320.jpg)









![Case #4:
• Available data: pH=7.53, PaCO2=12;
Na+
=140, K+
=3.0, Cl-
=106, HCO3=10
• Are the data internally consistent?
[ ] −
+
×=
3
2
24
HCO
PaCO
H](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-93-320.jpg)
![Case #4:
• [H+]~29, so pH~7.51; data consistent
• What is the primary disturbance?
• “__________ Alkalosis”
• Which variable (PaCO2, HCO3) is deranged
in a direction consistent with alkalosis?
∀↓ed PaCO2, ↓ed HCO3; so “Respiratory
Alkalosis”](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-94-320.jpg)
![Case #4:
• Is compensation appropriate?
• Acute respiratory alkalosis
– Plasma [HCO3] should fall by ~1-3 mmole/l for
each 10 mm Hg decrement in PaCO2, usually
not to less than 18 mmoles/l
• PaCO2 ↓ed by ~30 mm Hg; HCO3 should
fall by 3-9 mmole/l; HCO3 ↓ is too great, so
superimposed metabolic acidosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-95-320.jpg)


![Case #5:
• Are the data consistent?
• [H+
]=122, pH~6.9; data are consistent
[ ] −
+
×=
3
2
24
HCO
PaCO
H](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-98-320.jpg)

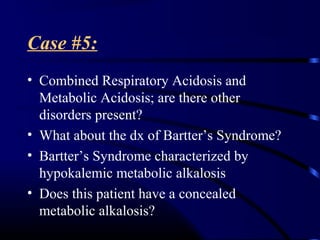
![Case #5:
• Acute Respiratory Acidosis
– Plasma [HCO3] should rise by ~1mmole/l for
each 10 mm Hg increment in PaCO2
• Since HCO3 is inappropriately depressed,
compensation is not appropriate, and there
is a concomitant metabolic acidosis as well
• What is the anion gap?
• AG=39, confirms metabolic acidosis](https://image.slidesharecdn.com/acidbasevijish-180217085957/85/Acid-base-A-B-G-100-320.jpg)















The document provides information on interpreting arterial blood gases (ABGs), including: - An ABG test measures pH, oxygen and carbon dioxide levels to assess acid-base and ventilation status. - Normal ABG values are provided as well as how to identify simple acid-base disorders based on pH, PCO2 and HCO3 levels. - Examples of ABG reports are given along with analyzing what abnormalities are present and what actions should be taken, such as adjusting ventilator settings or oxygen levels. The importance of clinical context is also stressed.