Download to read offline


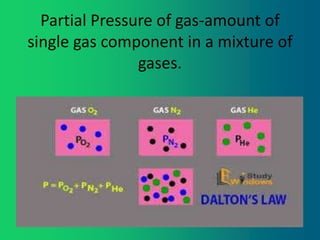
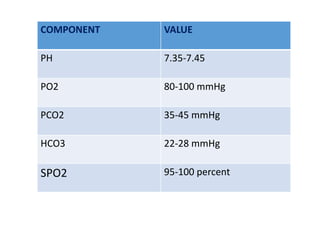
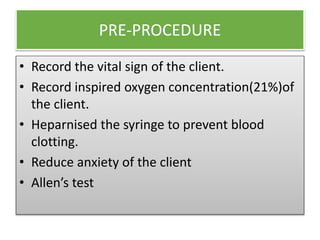
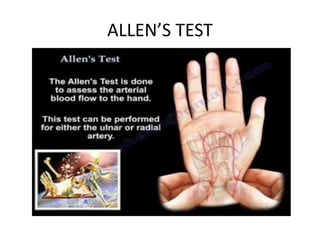
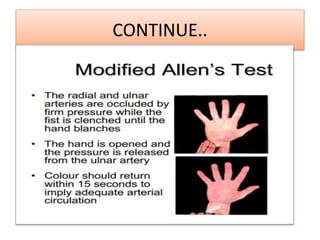
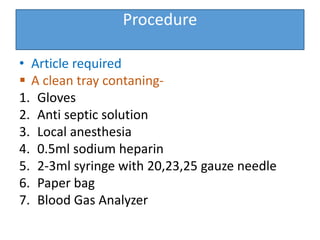
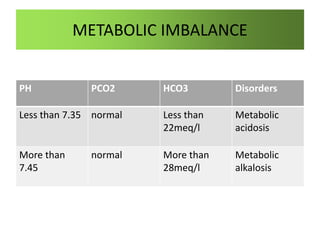


The document presents a detailed overview of arterial blood gas (ABG) analysis, including its definition, purposes, indications, and procedure for conducting the test. It outlines the components of ABG, their normal values, and potential complications, as well as methods for interpreting results related to acid-base imbalances. Additionally, it provides references for further reading and guidelines for ensuring proper technique during the procedure.






































![ARTERIAL BLOOD GAS [ABG] ANALYSIS PURPOSES, PROCEDURES](https://cdn.slidesharecdn.com/ss_thumbnails/arterialbloodga1-250329163652-107ce59f-thumbnail.jpg?width=640&height=640&fit=bounds)








![ABG[1].pptx BY DR BHAWNA ESI PGIMSR, BASAIDA](https://cdn.slidesharecdn.com/ss_thumbnails/abg1-250915145144-de471f3c-thumbnail.jpg?width=640&height=640&fit=bounds)



























