Downloaded 307 times
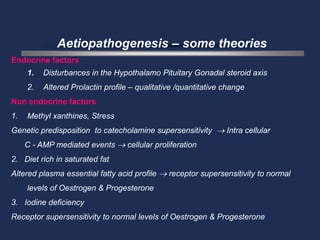
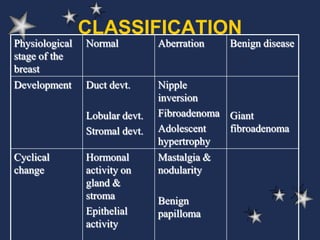
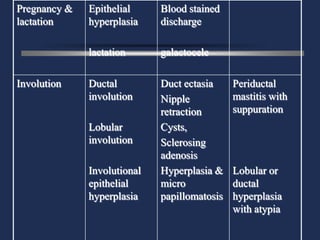
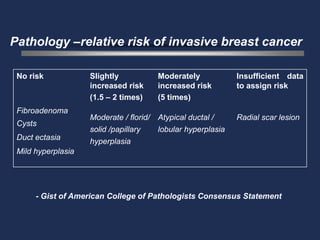
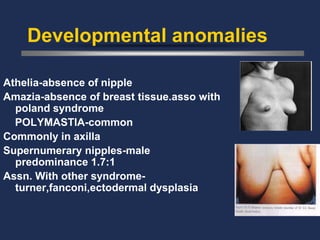
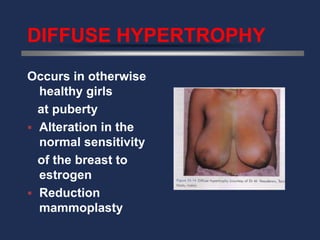
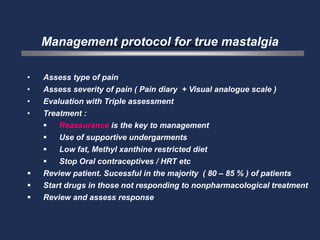
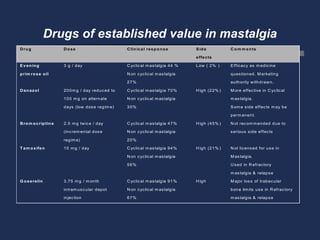
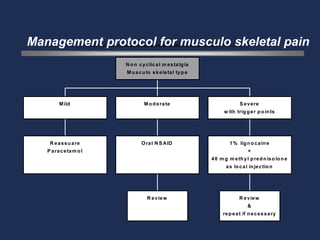
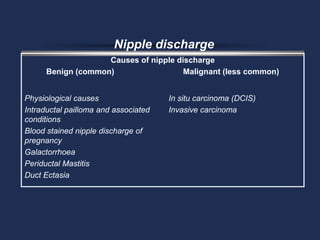
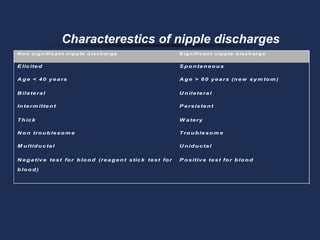
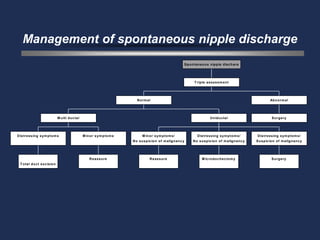
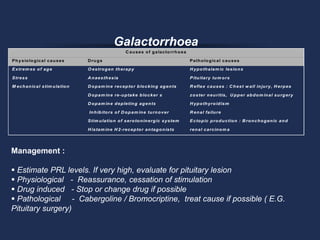
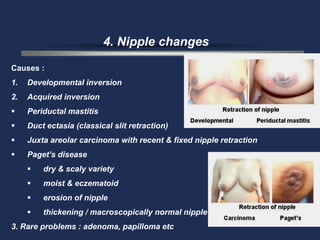
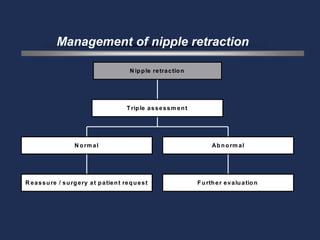

This document describes aberrations in normal breast development and involution. It discusses various benign and malignant conditions that can occur, including lumps, pain, nipple discharge, galactorrhea, and nipple changes. Potential causes are endocrine disturbances, genetic factors, environmental exposures, and developmental anomalies. Conditions range from near-normal to severe disease. Management depends on the condition but may include reassurance, lifestyle changes, medications, or surgery. Differentiating benign from malignant conditions requires evaluation using a triple assessment approach.





























































































