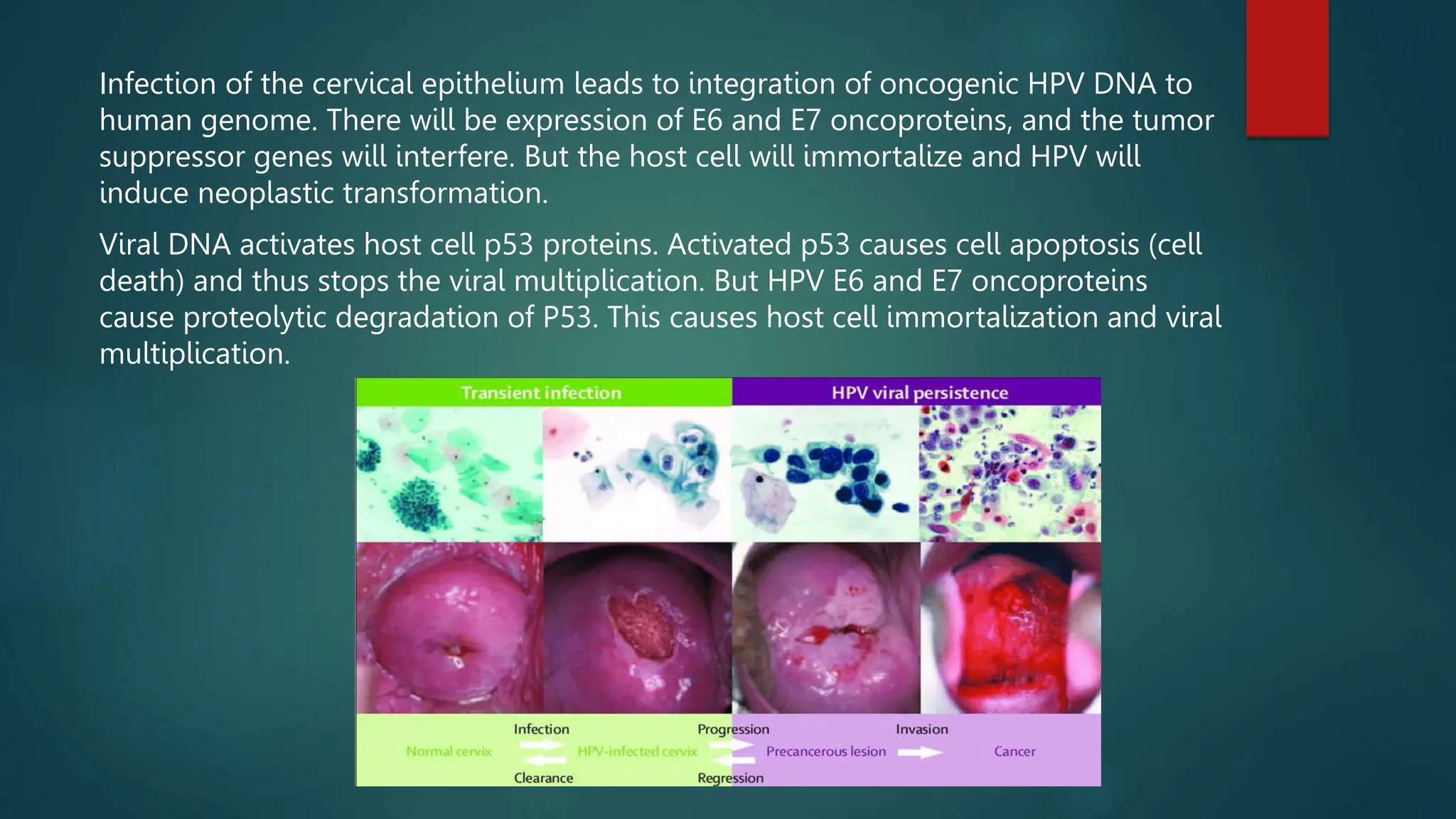
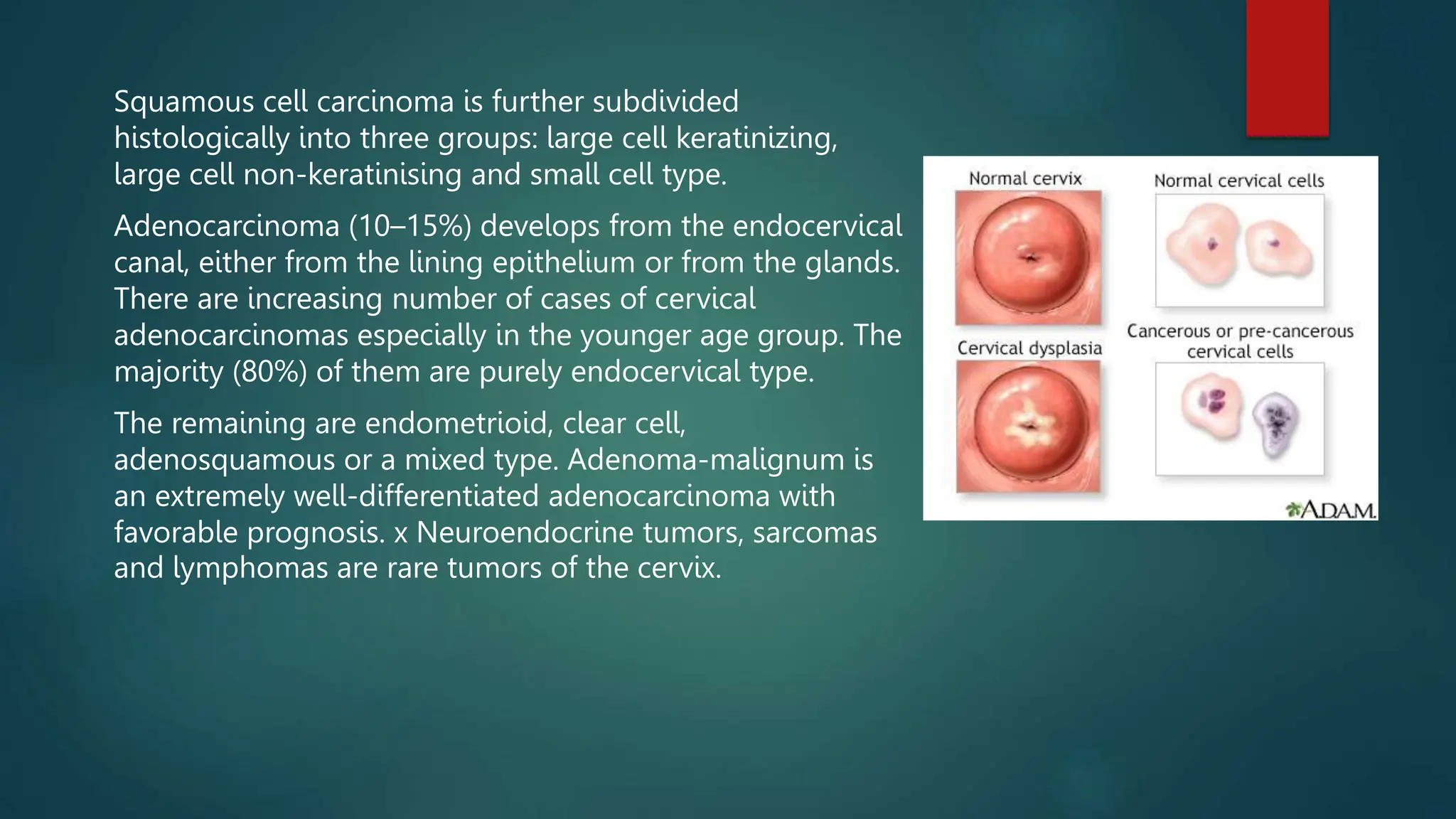
Cervical cancer occurs in the cervix and is mainly caused by HPV infection. Examination includes speculum exam to visualize lesions and biopsy for diagnosis. Risk factors include multiple sexual partners and smoking. Early symptoms may include abnormal bleeding but it can also be asymptomatic. Treatment depends on stage but may include surgery, radiation, chemotherapy, or a combination. Regular pap smears can help detect early changes. Vaccination and safe sex practices can help prevent HPV infection and therefore reduce cervical cancer risk.












































































![menstrual cycle [Autosaved]-2 (5).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/menstrualcycleautosaved-25-230321042311-7c0898c3-thumbnail.jpg?width=640&height=640&fit=bounds)






















