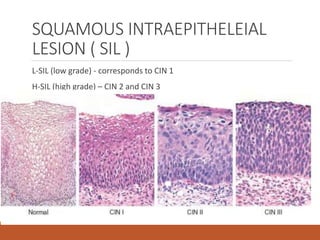
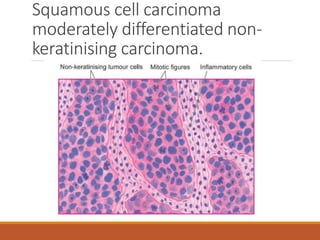
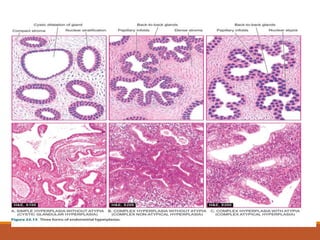
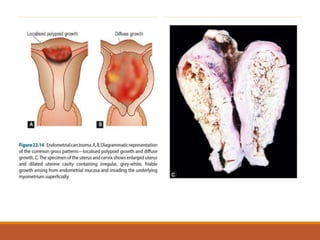
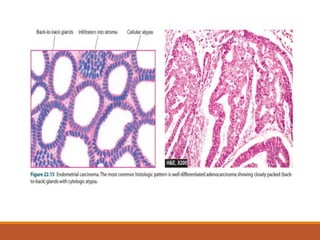
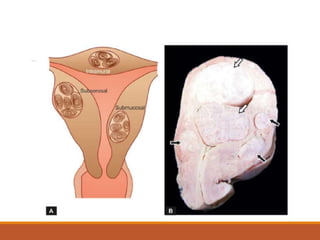
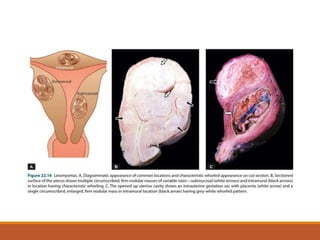
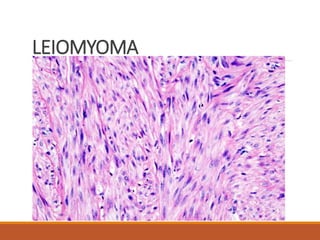
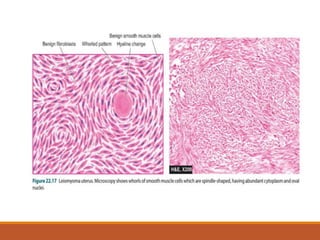
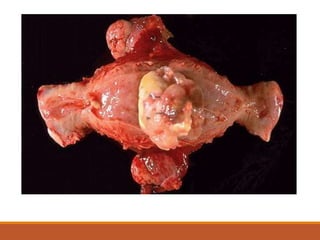
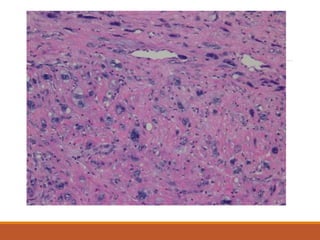
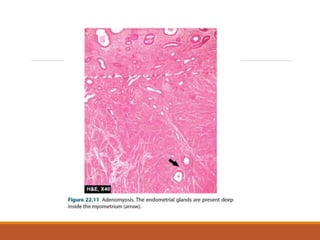
This document summarizes the anatomy and pathologies of the female genital tract. It describes the components of the FGT including the vulva, vagina, cervix, uterus, fallopian tubes, and ovaries. It then discusses various cervical conditions like CIN, SIL, and invasive cervical carcinoma. It also covers uterine conditions such as endometrial hyperplasia, endometrial carcinoma types 1 and 2, and leiomyoma. Other topics mentioned include adenomyosis, endometriosis, and endocervical polyp. Risk factors, clinical features, gross and microscopic findings are provided for each condition.













![Cytopathology Of Cerebrospinal Fluid[1]Power Point](https://cdn.slidesharecdn.com/ss_thumbnails/cytopathologyofcerebrospinalfluid1power-point-1230479978520994-2-thumbnail.jpg?width=640&height=640&fit=bounds)























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







