Downloaded 1,361 times
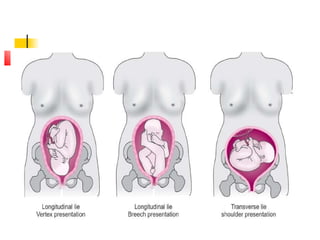

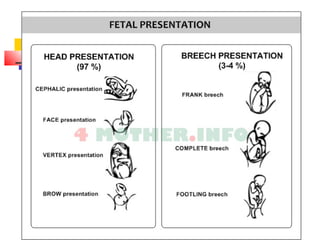

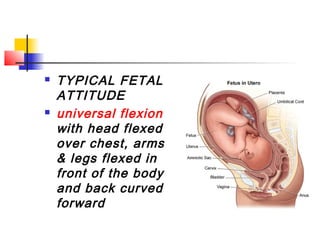

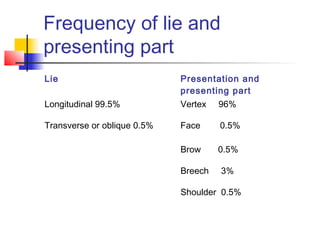
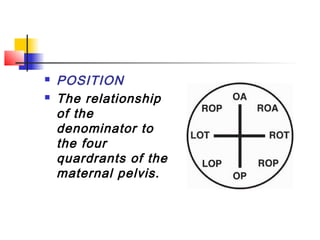


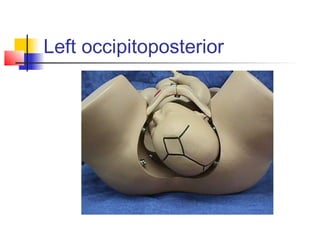

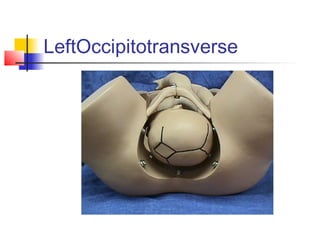
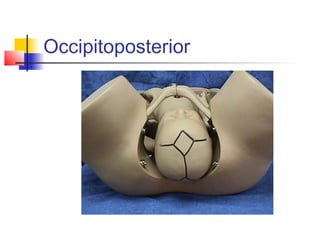


This document discusses the relationship between the fetus and the pelvis during childbirth. It describes the lie or orientation of the fetus, the presenting part of the fetus that engages the pelvis, and the position and attitude of the fetal head. The key points are: - The fetus most commonly lies longitudinally in the uterus with the head engaging the pelvis (cephalic presentation). - The position describes the location of the presenting part, such as the occiput, in relation to maternal pelvic quadrants. - The attitude refers to the flexion or extension of fetal parts. Flexion is most common with the head flexed forward onto the chest. - Moulding, or shifting of fetal























































































