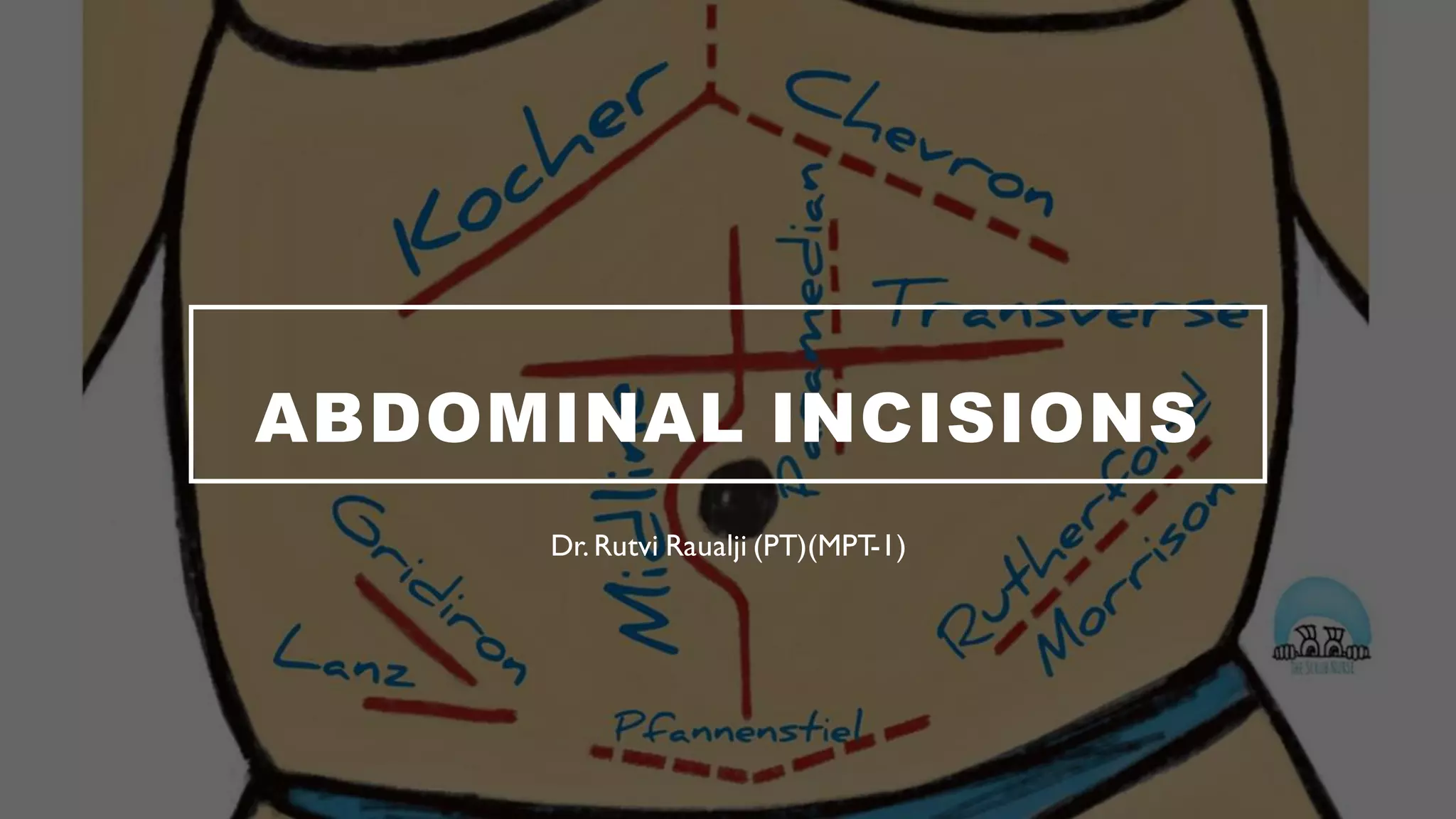
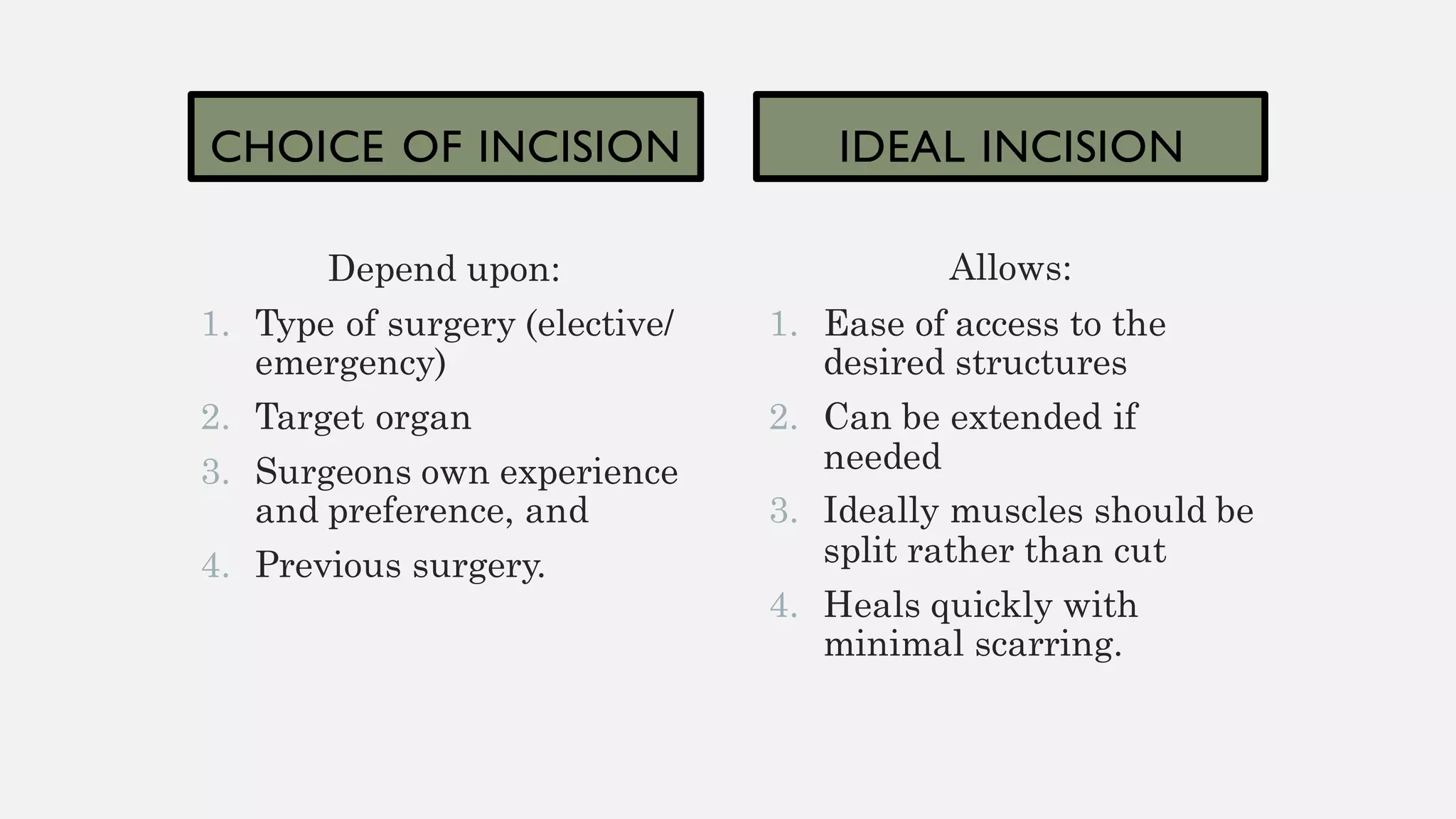
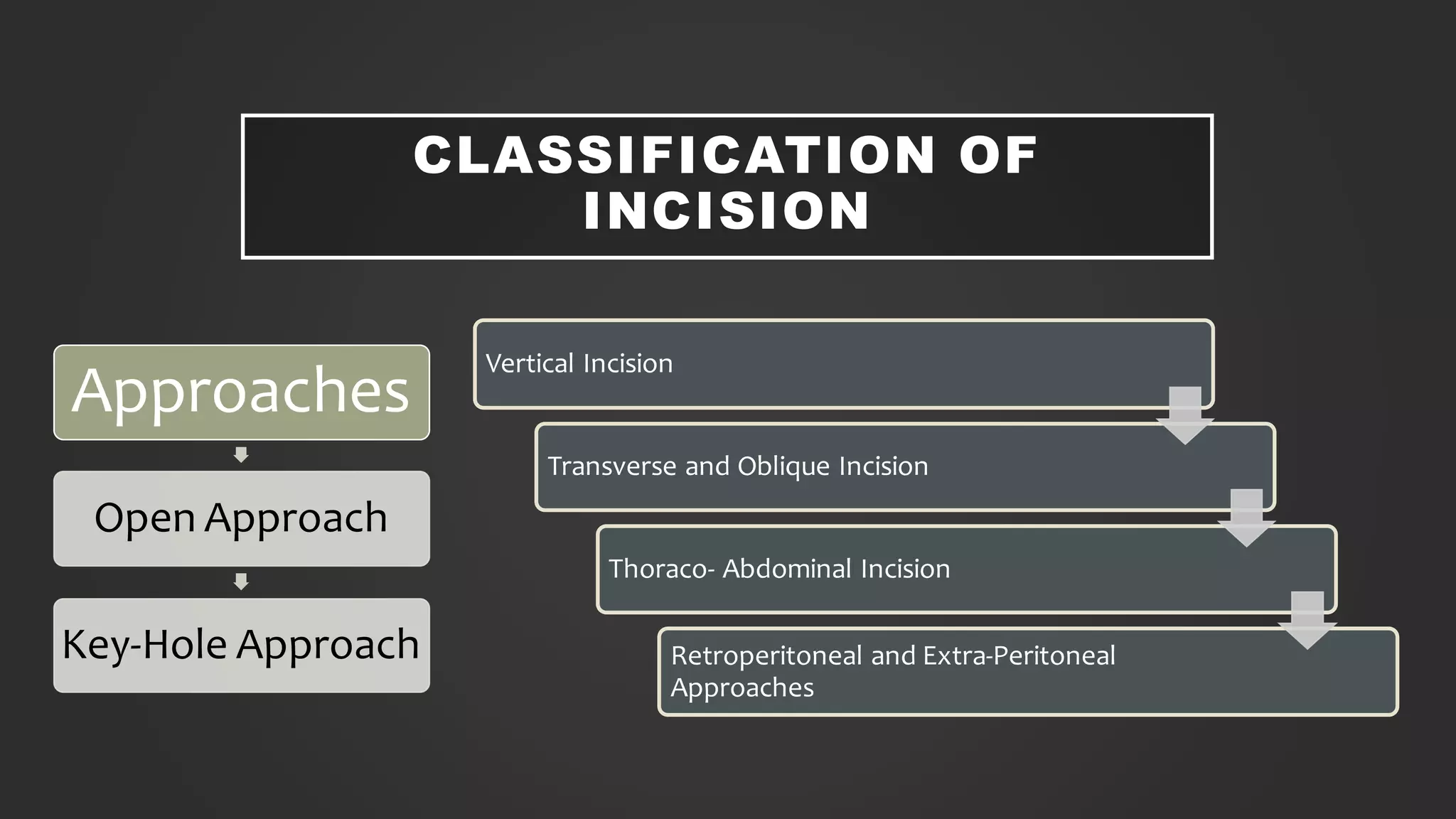
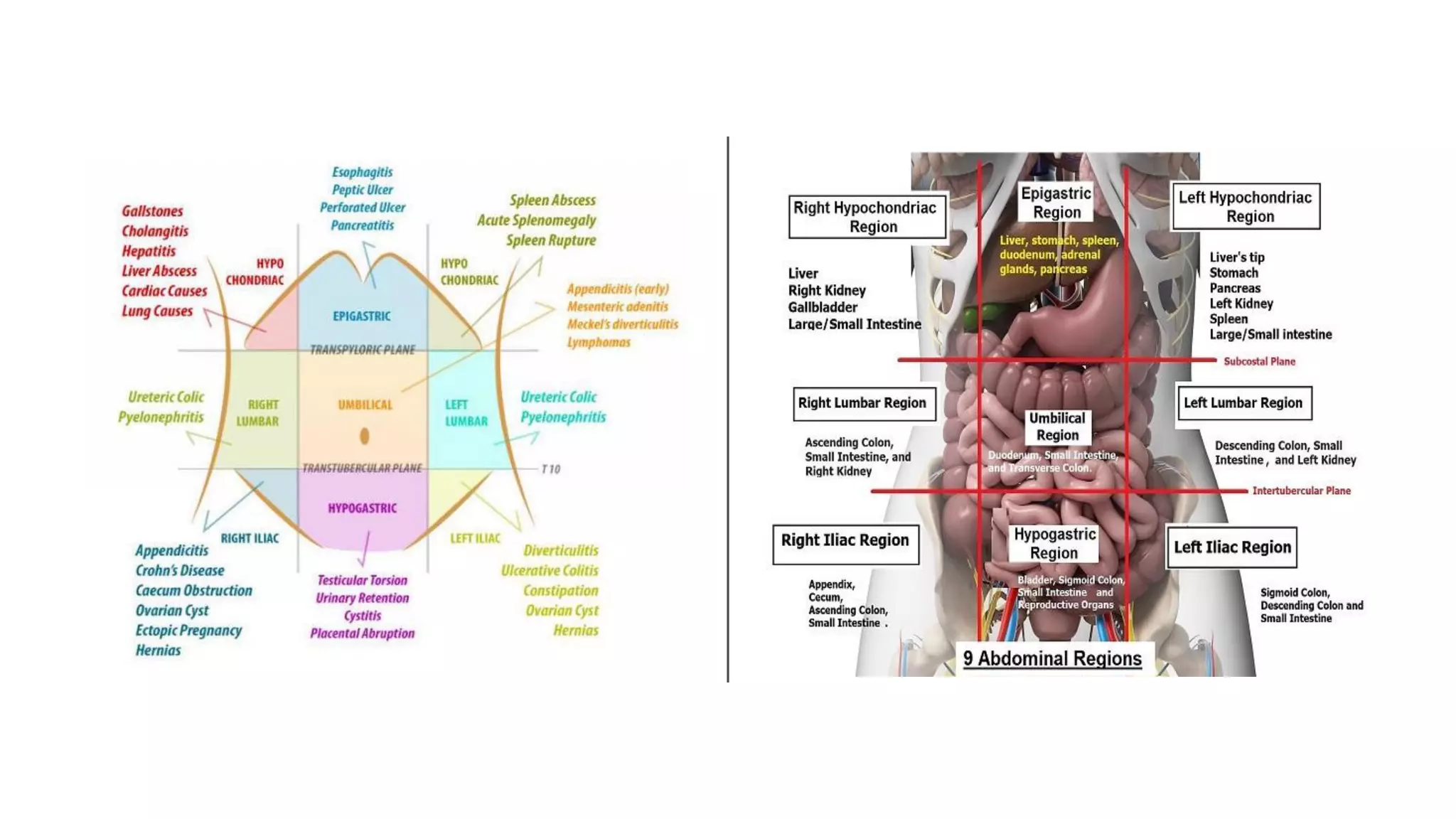
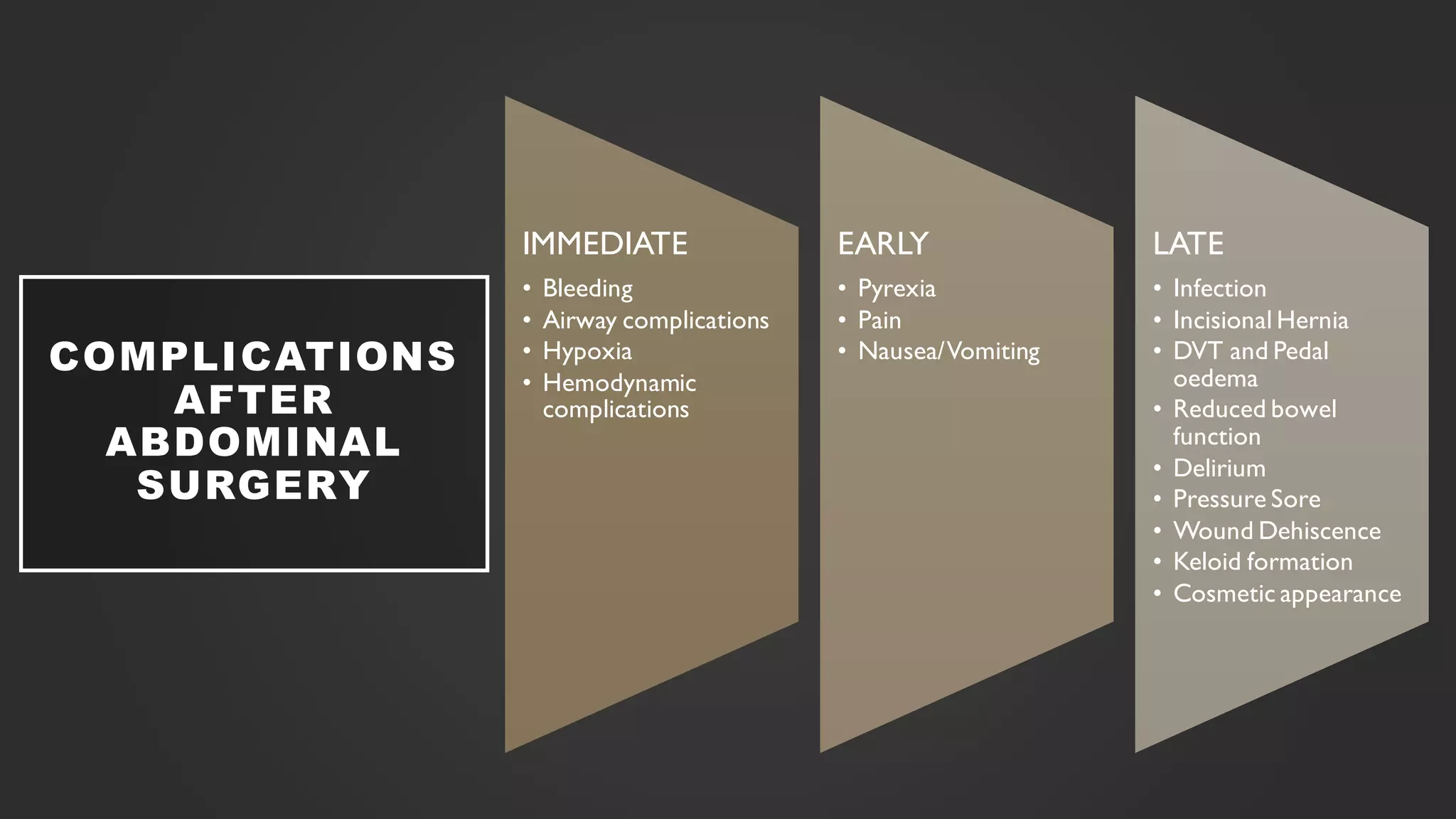
The document discusses various types of abdominal incisions used in surgery, highlighting the principles of incision selection, including accessibility, extensibility, and minimizing scarring. It categorizes incisions by type (vertical, transverse, and oblique) and their advantages and disadvantages, emphasizing the healing properties related to alignment with Langer's lines. Additionally, it outlines potential complications arising from abdominal surgery, both immediate and long-term.