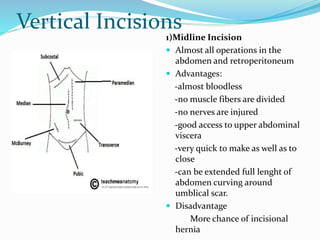
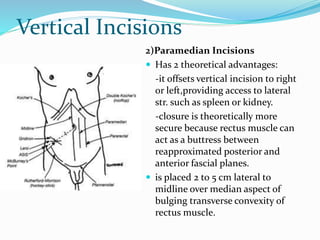
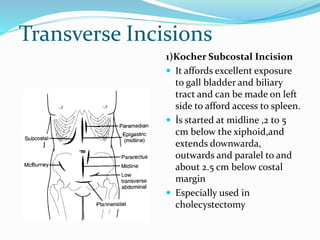
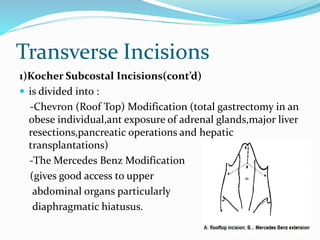
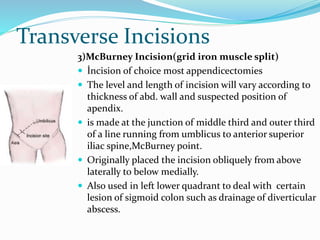
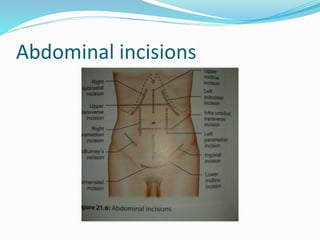
The document discusses various types of abdominal incisions used in surgery. It describes midline, vertical, transverse, and oblique incisions. Midline incisions provide good access but have a higher risk of hernia. Transverse incisions have better cosmetic outcomes and less risk of complications like hernia compared to vertical incisions. Specific incisions discussed include Kocher for gallbladder surgery, McBurney for appendicectomy, and Pfannenstiel for pelvic operations. Factors affecting incision healing and potential complications are also outlined.