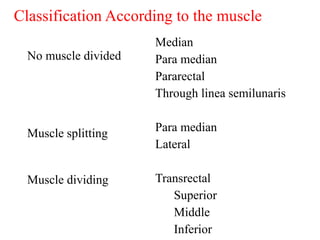
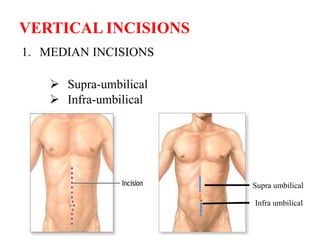
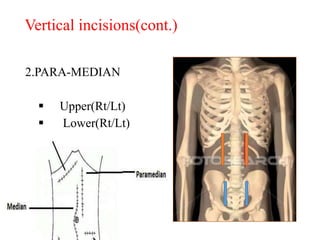
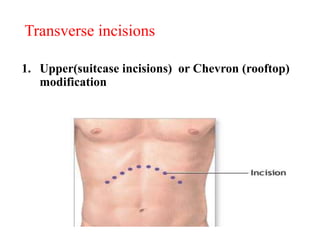
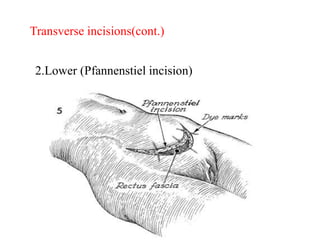
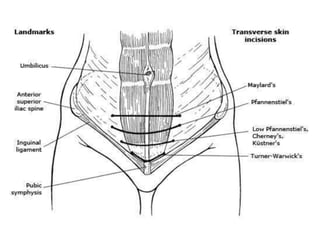
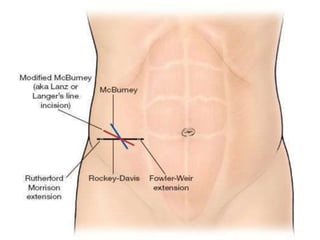
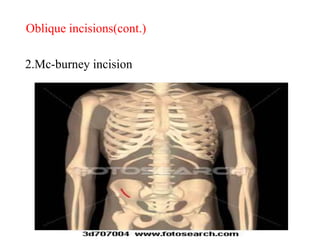
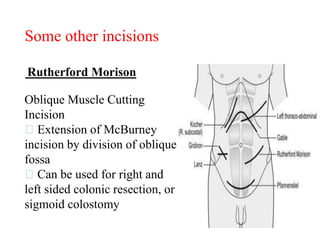
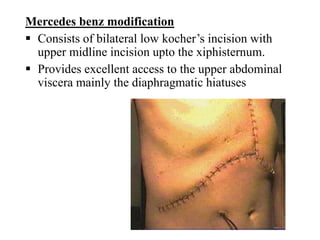
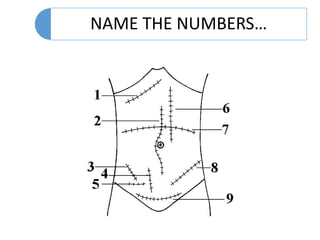
The document discusses various types of abdominal and thoracic surgical incisions. It describes incisions such as vertical (median, para-median), transverse (Pfannenstiel, Lanz), and oblique (Kocher, McBurney) incisions. Median incisions provide wide access to the abdominal cavity but have disadvantages like midline scarring. Para-median incisions provide lateral access but are cosmetically worse. Transverse incisions like Pfannenstiel are commonly used for gynecological and urological procedures. Oblique incisions give targeted access while minimizing muscle cutting.