Downloaded 250 times

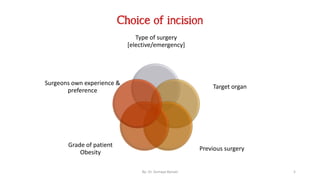
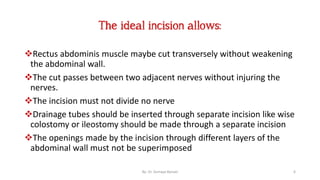
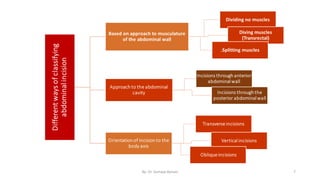
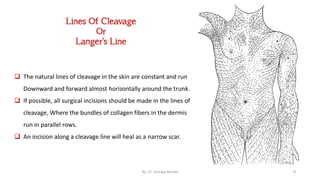
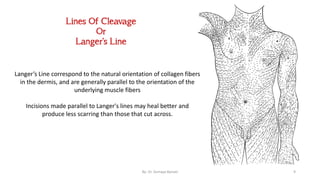
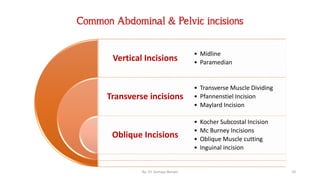
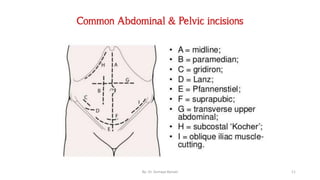
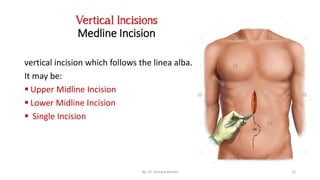
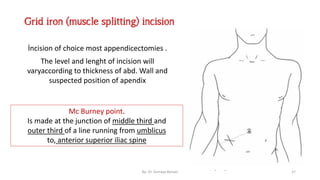
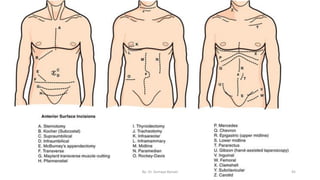

This document discusses surgical incisions, including: - The importance of choosing an incision that provides accessibility, extensibility, and security for the procedure. - Common abdominal and pelvic incisions such as vertical, transverse, oblique, midline, paramedian, Pfannenstiel, and flank incisions. - Factors to consider when choosing an incision, including the type of surgery, target organ, patient characteristics, and surgeon preference. - Principles for making incisions such as following skin cleavage lines and avoiding cutting nerves and vessels.













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


