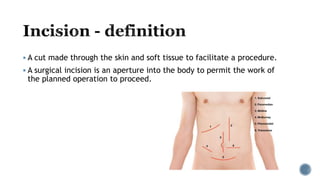
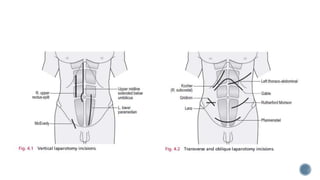
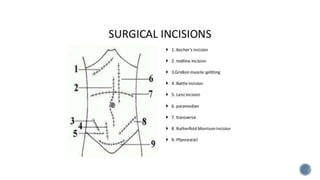
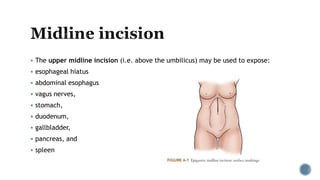
The document discusses various types of surgical incisions including vertical, transverse, and oblique incisions. It describes where each incision is made and what structures they provide access to. Some key incisions mentioned include midline, paramedian, subcostal, McBurney's, Pfannenstiel, and thoracoabdominal incisions. Factors to consider when choosing an incision include preoperative diagnosis, prior operations, and desired exposure and accessibility.



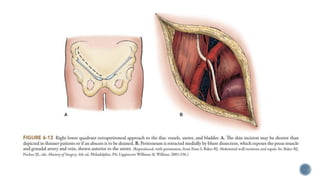
![ However, if palpation reveals a mass, the incision can be placed directly over the
mass.
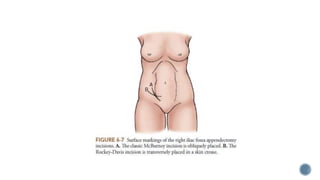
McBurney originally placed the incision obliquely, from above laterally to below
medially.
However, the skin incision can be placed in a skin crease transversely [Rockey-Davis
Incision or Lanz Incision or Bikini Incision]
It provides a better cosmetic result
(Delany & Carnevale, 1976; Pleterski & Temple, 1990)
Otherwise, the two incisions are similar.](https://image.slidesharecdn.com/abdominalincisions-230308170158-f483fe64/85/Abdominal-Incisions-pptx-38-320.jpg)