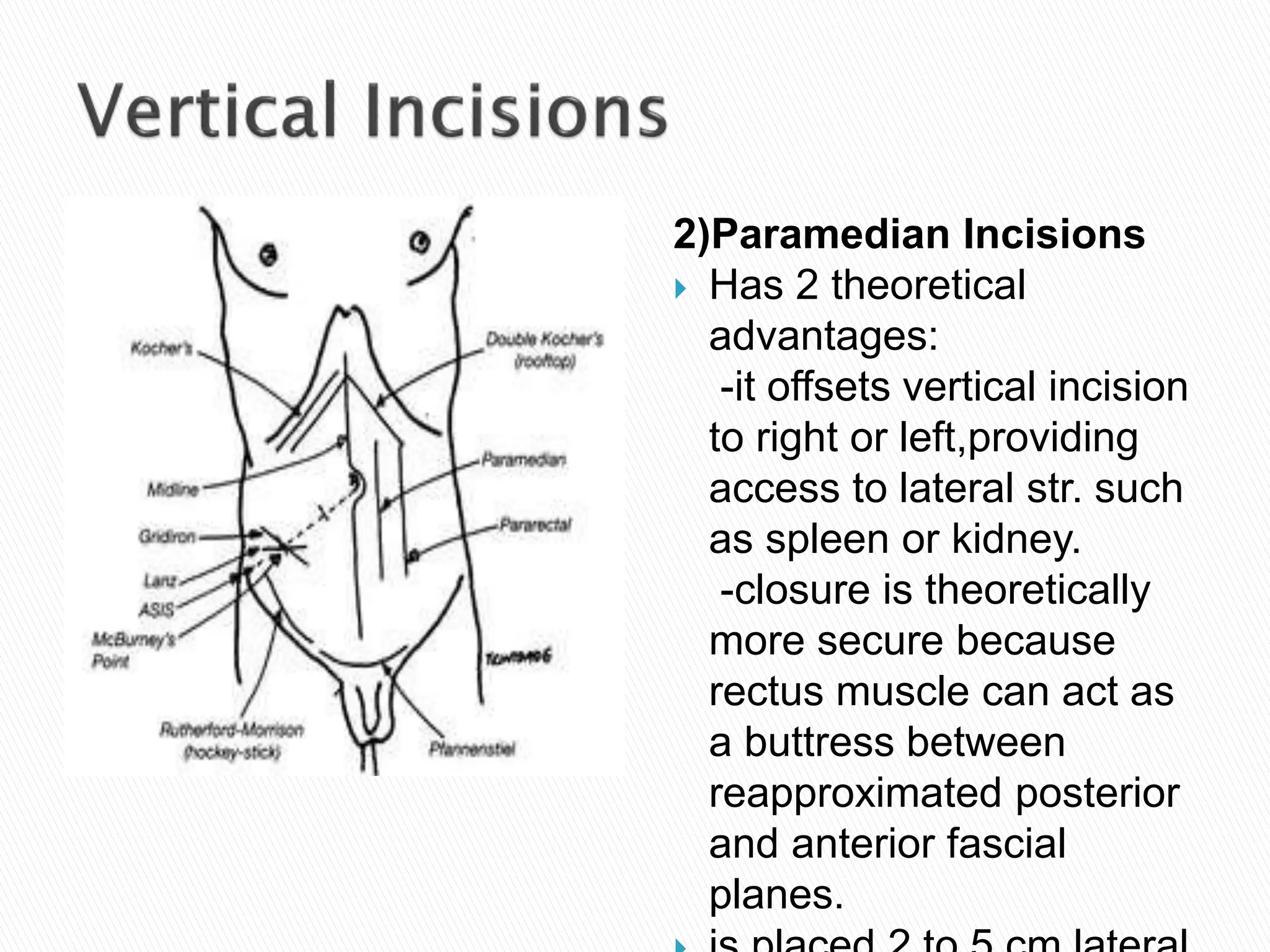
The document discusses various types of surgical incisions including their purposes, advantages, and disadvantages. It describes abdominal and pelvic incisions such as midline, paramedian, transverse, oblique, Kochler subcostal, McBurney, Pfannenstiel, and Maylard incisions. Langer's lines, which correspond to the natural orientation of collagen fibers, are also mentioned as incisions made parallel to these lines may result in better healing and less scarring. Key layers of the abdominal wall including skin, fascia, muscles and peritoneum are also defined.