The document discusses antenatal exercise and its importance during pregnancy, highlighting potential risks, benefits, and guidelines for safe physical activity. It covers various exercises for different stages of pregnancy and postpartum recovery, including pelvic floor training, posture improvement, and circulation enhancement, while addressing contraindications and warning signs. The content emphasizes the need for medical consent and tailored exercise regimens to support maternal health and wellbeing.






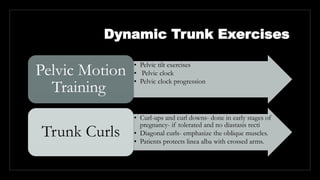
![Pelvic Motion Training (back pain; proprioceptive
awareness; lumbar, pelvic and hip mobility)
PELVIC TILT
EXERCISE: Quadruped
Position- posterior pelvic
tilt- isometric contraction of
lower abdominals- hold-
release and anterior pelvic
tilt.
PELVIC CLOCK: Hook
lying position- Umbilicus
[12] and pubic symphysis
[6]- gentle movements back
and forth [12-6] (basic pelvic
tilts)- then weight
shift to left hip and right hip
[3-6]- later, move in
clockwise and anti-clockwise.
PELVIC CLOCK
PROGRESSIONS: Cut the
clock in half [right-left/ up-
down]- move the pelvic in
arc on one side and back
through the middle. Later
counterclockwise motions
done.](https://image.slidesharecdn.com/antenatalexecrises-221024151945-4e7fa754/85/Antenatal-Execrises-pptx-15-320.jpg)
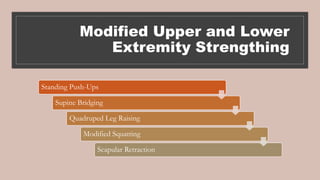
![STANDING
PUSH-UPS
Standing, facing wall, feet
pointed straight forward,
shoulder-width apart, arm
length away from wall-
palms placed at shoulder
height- woman slowly bends
the elbow, bring upper body
close to the wall (trunk and
pelvis stable), and heels on
the floor. Slowly pushes
with arm back to her
original position.
SUPINE
BRIDGING
Supine in hook
lying position –
posterior pelvic tilt
and then lifting
pelvis off the floor
Proression- holding
the position and
alternatly flexing
and extending
upper extremeties.
Emphasizes
stabilization of hip
extentors and trunk
musculature.
QUADRUPED
LEG
RAISING
Patient on hands and
knees- posterior pelvic
tilt and raising one LE
at the level no higher
than pelvis- slowly
lowering that leg and
repeating same on
opposite side.[NOTE:
Discontinue if pain
over SI joint]](https://image.slidesharecdn.com/antenatalexecrises-221024151945-4e7fa754/85/Antenatal-Execrises-pptx-17-320.jpg)

![Guidelines/ Dosage
§Medical Consent
§Gradually increase exercise if previously sedentary
§Frequency- 3 times a week
§Intensity- 25 to 30% of maximum heart rate [HRmax= 220- age (in years)]
§Type- Warm up, Conditioning (Moderate exercise) and Cool down
§Time- 30 to 45 mins ( 20 mins conditioning duration)](https://image.slidesharecdn.com/antenatalexecrises-221024151945-4e7fa754/85/Antenatal-Execrises-pptx-29-320.jpg)