Downloaded 294 times
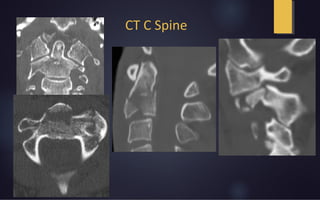
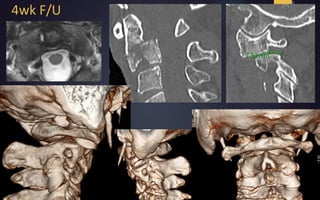
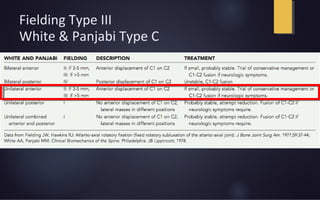
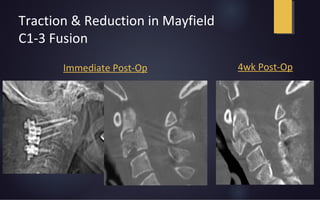

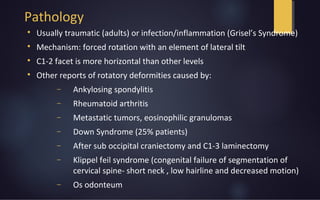
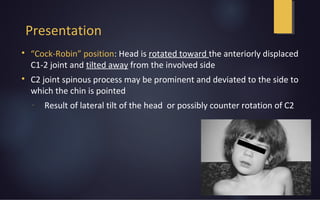
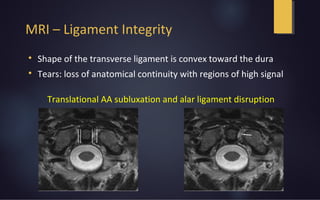
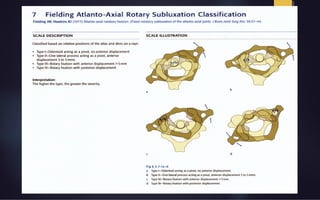



A 64-year-old male presented with neck pain after falling down stairs while intoxicated. Imaging showed posterior interspinous ligament edema and fluid in the C1-C2 articulations, consistent with traumatic atlantoaxial rotatory subluxation (Fielding Type III). The patient underwent traction and reduction followed by C1-C3 fusion. Atlantoaxial rotatory subluxation occurs when forced rotation combines with lateral tilt, placing stress on ligaments like the transverse ligament. It can be caused by trauma, infection, arthritis or other conditions. Imaging helps identify ligament disruption and bone displacement. Surgical fusion is often needed for stabilization.























































































