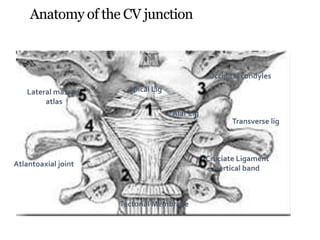
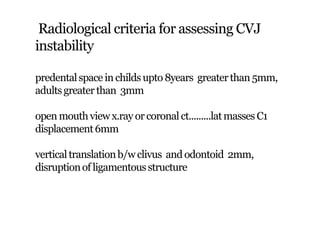
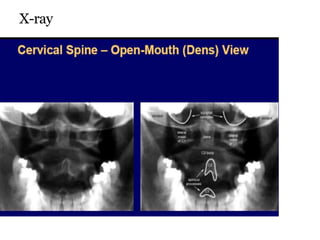
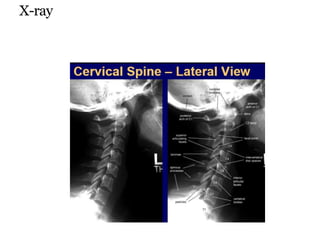
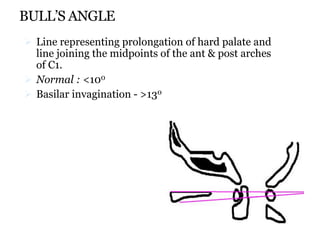
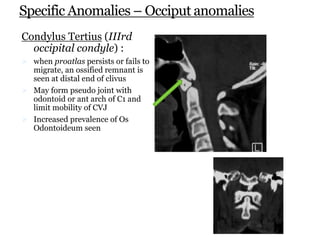
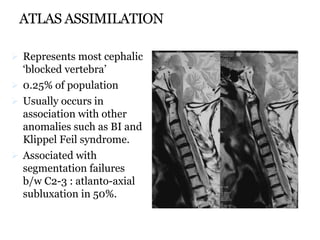
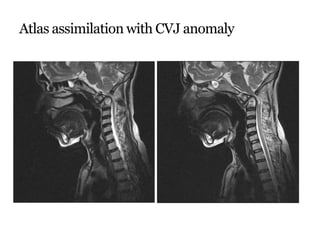
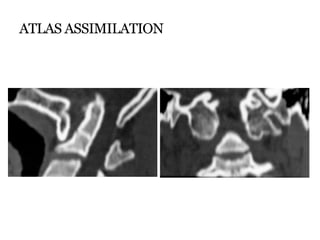
This document discusses abnormalities of the craniovertebral junction (CVJ). It begins by defining the anatomical structures that make up the CVJ. It then covers the embryology and normal anatomy, including range of motion measurements. Radiological assessment criteria are outlined. Various congenital and acquired disorders are described such as basilar invagination and atlantoaxial subluxation. Specific conditions involving the occiput, atlas, and odontoid are also detailed.
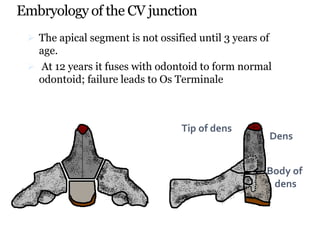





















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


