ANATOMY OF CERVICALSPINE
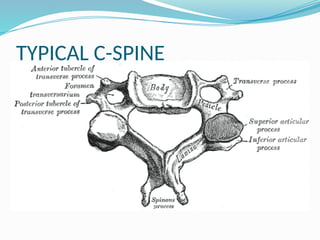
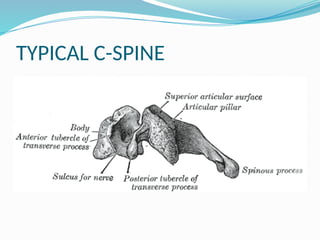
Typical vertebrae [ C3- C6 ]
Atypical vertebrae
Atlas
Axis
C 7
3.
ATLAS
No bodyand spinous process, consists of 2 lateral
masses.
Short Anterior & long posterior arches
Transverse ligament – strong ligament, retains
the dens process.
4.
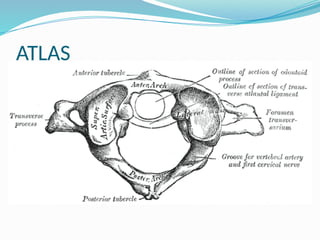
ATLAS
Lateral mass-bears reniform sup articular facet
Inf articular facet- circular, medial & backward
Posterior arch- 3/5ths of circumference, sup
surface groove for vertebral A., attachment to
post atlanto-occipital membrane, inf border to lig
flavum
Posterior tubercle- ligamentum nuchae, rectus
capitis posterior
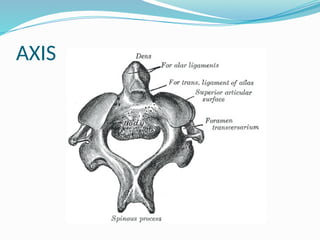
AXIS
Salient featureis the DENS (odontoid process)
Conical shape , mean length 15mm
3 parts- Apex, waist & base
Apex- pointed, apical & alar ligaments
Ant surface- ovoid articular facet
Post surface grooved by transverse ligament
7.
AXIS
Pedicle –thick, covered by sup articular facet
Inf facet is typical
Laminae thick due to muscle attachments
Massive spinous process
Transverse process has no ant. tubercle
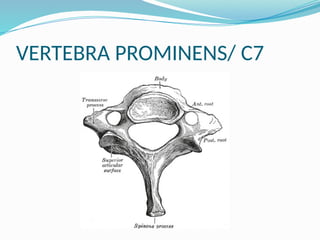
VERTEBRA PROMINENS/ C7
Spinous process is long & non-bifid
Attachment to trapezius, spinalis capitis,
mutifidus, interspinales
Transverse process lacks ant tubercle
Foramen transversarium transmits only veins
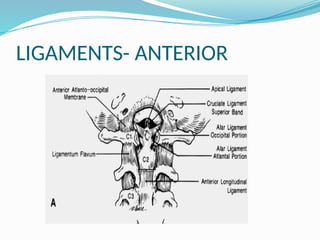
LIGAMENTS
Anterior group:A.L.L. ascends as atlanto-
occipital membrane, P.L.L ascends as tectorial
membrane
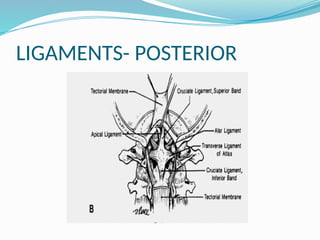
Posterior group:
Supraspinous ligament- head in extension
Interspinous ligament
Ligamentum flavum- head in flexion
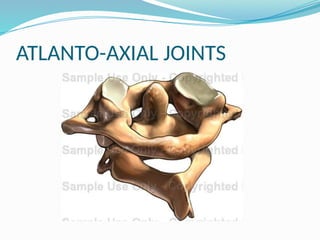
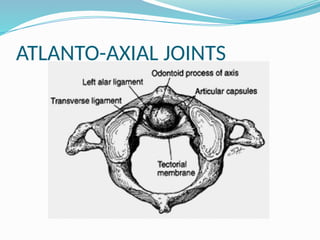
ATLANTO-AXIAL JOINTS
3synovial joints- pair between lateral masses,
median complex between dens & anterior arch
of atlas.
Lateral atlanto- axial joint: reciprocally concave
in coronal plane, accessory ligament stabilizes
Medial atlanto-axial joint: pivot joint, vertically
ovoid facet on dens articulates with ant arch,
also with transverse ligament
MOVEMENTS AT ATLANTO-AXIALJOINTS
Simultaneous at all 3 joints
Exclusively rotation of axis
Axis ascends into atlantal ring during rotation
22.
ATLANTO- OCCIPITAL JOINT
Connected by capsule, anterior & posterior
atlanto occipital membrane
Anterior atlanto occipital membrane- connects
anterior margin of foramen magnum to upper
border of ant arch, strengthened by ALL
Posterior atlanto occipital membrane- post
margin of foramen magnum to post arch
23.
EPIDEMIOLOGY OF CERVICALINJURIES
Bimodal age distribution- adolescents/young
adults (15 to 24 years old) and middle-aged
individuals (over 55 years old).
The upper cervical vertebrae (C1 and C2) are the
most frequent.
24.
PREHOSPITAL CARE
Carefor a patient with a potential cervical spine
injury begins in the field.
Manual immobilization of the head and neck
should be maintained until a hard cervical collar
can be applied.
NecLoc collar, Miami J, Philadelphia, Aspen, and
Stifneck devices, application of Gardner-Wells
tongs and traction.
25.
IN-HOSPITAL RESUSCITATION
Initialassessment of the ABCs .
The neck should be immobilized by manual in-
line stabilization during transfers.
26.
The patientcan be moved between the stretcher
and bed using a rigid transfer board.
Log-roll technique and spinal precautions
should be observed at all times.
Patients with spinal cord injury often present
with neurogenic shock.
Neurogenic shock results in hypotension
accompanied by bradycardia.
27.
Pressure shouldbe restored by a combination of
postural maneuvers (Trendelenburg position),
judicious fluid infusion, and vasopressor
administration.
28.
HISTORY
Previous injuries,the nature of the current
injury, and where he or she is feeling pain,
Concomitant distracting injuries, the direction of
impact should be asked.
29.
PHYSICAL EXAMINATION
spineshould be examined in a systematic
manner.
The spinous processes should be palpated
individually, noting tenderness, crepitus, or step-
off.
Bruising or laceration should be noted.
Rotation of the head and neck should be noted-
unilateral facet dislocations.
30.
A detailedneurologic examination is performed
in the awake, alert patient.
31.
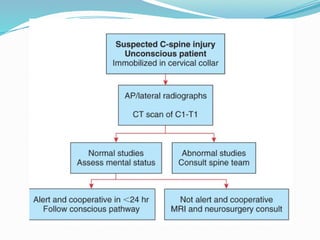
In thenonalert patient, the neurologic
examination is limited, Key components can still
be peformed.
Rectal tone, bulbocavernosus (BC) reflex should
also be noted and documented.
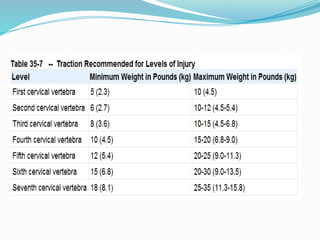
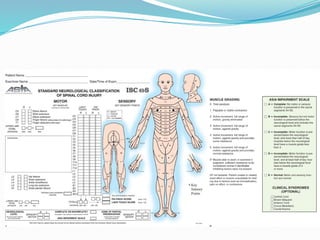
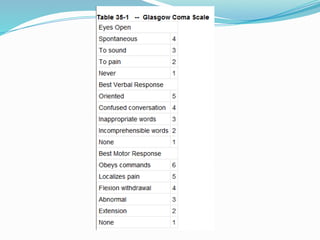
36.
Initial Imaging Protocol
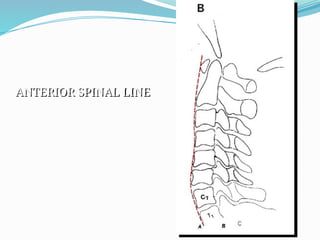
A lateral cervical radiograph is a standard
component of the general trauma series .
This view is useful in detecting up to 85% of
cervical spine injuries.
A standard cervical series includes a lateral,
anteroposterior (AP), and open-mouth
views(83% and 99% of injuries can be detected).
37.
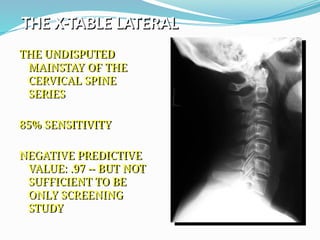
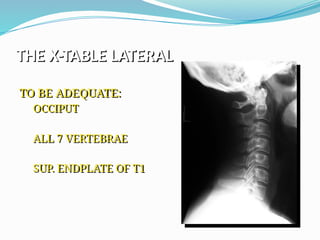
THE X-TABLE LATERAL
THEUNDISPUTED
MAINSTAY OF THE
CERVICAL SPINE
SERIES
85% SENSITIVITY
NEGATIVE PREDICTIVE
VALUE: .97 -- BUT NOT
SUFFICIENT TO BE
ONLY SCREENING
STUDY
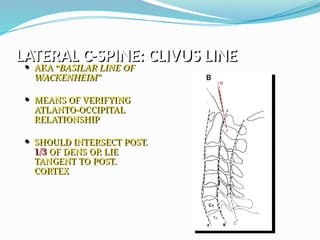
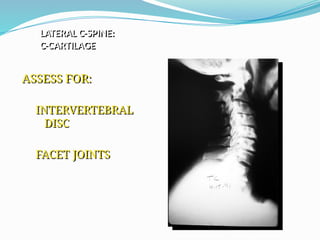
LATERAL C-SPINE: CLIVUSLINE
AKA “BASILAR LINE OF
WACKENHEIM”
MEANS OF VERIFYING
ATLANTO-OCCIPITAL
RELATIONSHIP
SHOULD INTERSECT POST.
1/3 OF DENS OR LIE
TANGENT TO POST.
CORTEX
45.
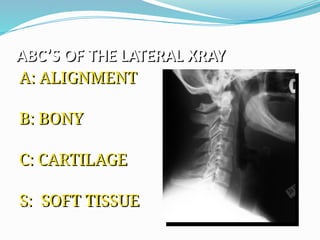
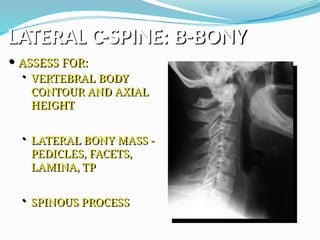
LATERAL C-SPINE: B-BONY
ASSESS FOR:
• VERTEBRAL BODY
CONTOUR AND AXIAL
HEIGHT
• LATERAL BONY MASS -
PEDICLES, FACETS,
LAMINA, TP
• SPINOUS PROCESS
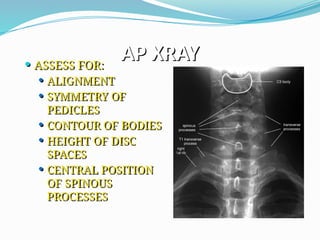
AP XRAY
ASSESSFOR:
ALIGNMENT
SYMMETRY OF
PEDICLES
CONTOUR OF BODIES
HEIGHT OF DISC
SPACES
CENTRAL POSITION
OF SPINOUS
PROCESSES
49.
AP XRAY
FACET JOINTSORIENTED AT 45 DEGREE
ANGLE FROM CORONAL PLANE -- THUS NOT
SEEN ON AP
IF FACET IS CLEARLY IDENTIFIED ON AP,
ARTICULAR PILLAR OR PEDICLE FX WITH
ROTATION IS LIKELY
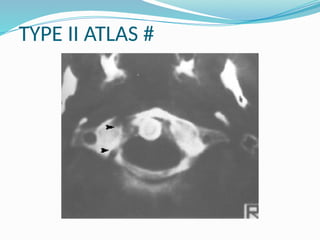
OCCIPITAL CONDYLE #
Two types of injuries
First is axial compression causing impaction or
fracturing of the articular surface.
Fractures within the atlanto-occipital joint may
occur when extremes of rotation cause avulsion
of articular surface by the alar ligaments.
54.
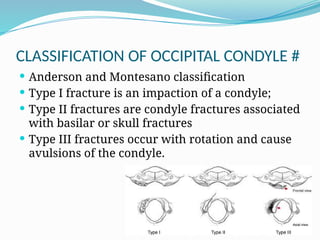
CLASSIFICATION OF OCCIPITALCONDYLE #
Anderson and Montesano classification
Type I fracture is an impaction of a condyle;
Type II fractures are condyle fractures associated
with basilar or skull fractures
Type III fractures occur with rotation and cause
avulsions of the condyle.
55.
TREATMENT OF OCCIPITALCONDYLE #
Type I & II – stable injuries- can be treated in
rigid cervical orthosis for 8 wks
Type III- potentially unstable, avulsion of alar
ligaments, immobilization for 12 wks in halo
vest
If unstable even after this – occipital to C2 fusion
56.
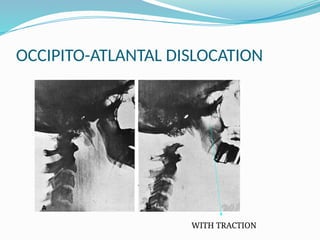
OCCIPITO-ATLANTAL DISLOCATION
High-energymotor vehicle accidents and
usually present with multiple injuries.
The dislocation is said to result from a
combination of hyperextension, distraction,
and rotation of the craniocervical junction.
Severe neurologic injuries ranging from
complete C1 level flaccid quadriplegia to
mixed incomplete spinal cord syndromes such
as Brown-Séquard syndrome and cruciate
paralysis.
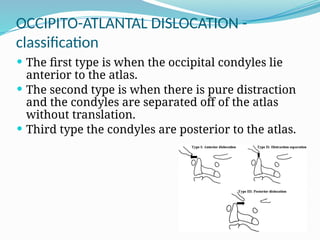
OCCIPITO-ATLANTAL DISLOCATION -
classification
The first type is when the occipital condyles lie
anterior to the atlas.
The second type is when there is pure distraction
and the condyles are separated off of the atlas
without translation.
Third type the condyles are posterior to the atlas.
59.
TREATMENT
Careful applicationof the halo and placement of
the halo vest.
Attempts of reduction should be undertaken
with great care and preferably with fluoroscopic
guidance.
Since this injury results almost wholly from
ligamentous failure, occipitocervical fusion is
required for long-term stability.
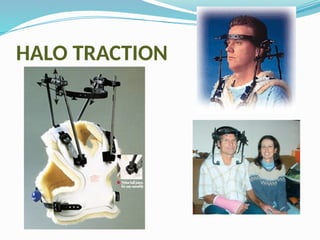
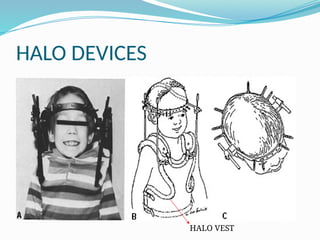
HALO DEVICE
Firstused by Perry & Nickels in 1959
Halo selected held below area of greatest
diameter of skull at level of eyebrows & 1cm
above ear level.
Introduce pins & tighten 2 diagonally opposite
pins simultaneously.
Secure pins to halo with lock nuts & attach halo
ring to vest through ant & post uprights.
62.
FRACTURES OF ATLAS
Fractures of the C1 vertebra or atlas occur
predominately through axial compression injuries.
Variations in fracture types may occur if the force is
applied symmetrically across both occipital condyles
onto the atlas or if the force is asymmetric.
The addition of an extension force can alter the
nature of the injury.
Symptoms- neck pain, instability, neurologic
weakness(rare).
63.
FRACTURES OF ATLAS
Based on mechanism of injury.- 3 types.
Direct, symmetric axial compression, the
ring of the atlas can fracture in three or four
locations, thus forcing the lateral masses
apart. This is called a Jefferson fracture
The second type of atlas fracture occurs when
an asymmetric axial force fractures the arch
immediately anterior to and posterior to one
of the lateral masses and displaces it
Finally, the posterior arch can fracture when
hyperextension is the major vector.
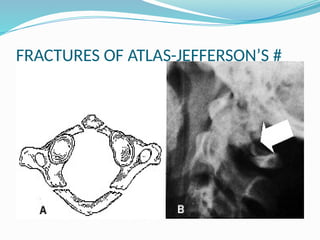
JEFFERSON’S #
Burst# of ring of atlas
Axial loading directed down on C1 ring
On AP view if lateral masses are >7mm wider
Undisplaced # - Halo device for 12 wks
Unstable # - occiput to C2 arthrodesis
TREATMENT OF ATLAS#S
Treatment of atlas fractures depends on the relative
stability of the fracture pattern.
Stable fractures are either posterior arch fractures or
nondisplaced fractures involving the anterior and posterior
portion of the ring. These fractures can be treated with a
cervical orthosis.
Type II # - can be treated by rigid immobilization
Unstable #- occipito cervical fusion
68.
ATLANTO-AXIAL ROTATORY SUBLUXATION
The mechanism of injury in atlantoaxial rotatory
subluxation is unknown.
It can occur spontaneously or after trauma.
Patients complain of neck pain, occipital
neuralgia, and, occasionally, symptoms of
vertebrobasilar artery insufficiency.
69.
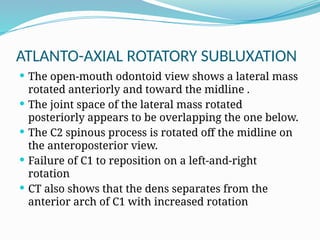
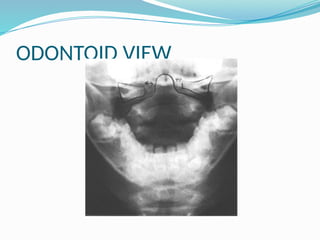
ATLANTO-AXIAL ROTATORY SUBLUXATION
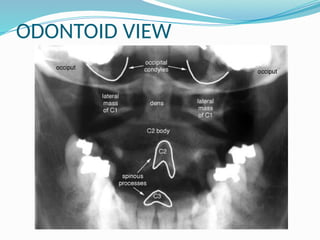
The open-mouth odontoid view shows a lateral mass
rotated anteriorly and toward the midline .
The joint space of the lateral mass rotated
posteriorly appears to be overlapping the one below.
The C2 spinous process is rotated off the midline on
the anteroposterior view.
Failure of C1 to reposition on a left-and-right
rotation
CT also shows that the dens separates from the
anterior arch of C1 with increased rotation
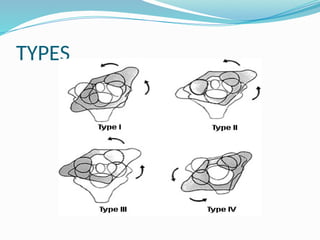
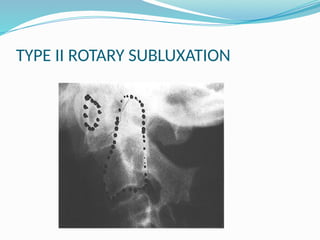
TYPES
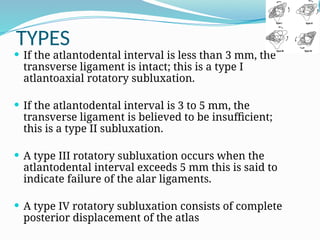
If theatlantodental interval is less than 3 mm, the
transverse ligament is intact; this is a type I
atlantoaxial rotatory subluxation.
If the atlantodental interval is 3 to 5 mm, the
transverse ligament is believed to be insufficient;
this is a type II subluxation.
A type III rotatory subluxation occurs when the
atlantodental interval exceeds 5 mm this is said to
indicate failure of the alar ligaments.
A type IV rotatory subluxation consists of complete
posterior displacement of the atlas
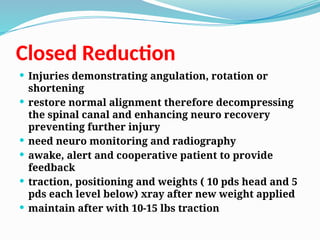
C1- C2 DISLOCATION
A]Forward dislocation with trans lig rupture
B] Forward subluxation with odontoid #
C] Posterior dislocation of atlas
D] Rotary subluxation
75.
TREATMENT
Treatment consistsof cervical halter traction in the
supine position and active rotation range-of-motion
exercises for 24 to 48 hours.
This is followed by ambulatory orthotic
immobilization with active range-of-motion
exercises until free motion returns.
Fixed rotation with continued symptoms and lack of
motion indicates a C1–C2 posterior fusion.
76.
FRACTURE OF ODONTOID
Dens fractures generally occur in high-energy
accidents involving motor vehicles or falls.
The rate of neurologic involvement ranges from
5% to 10% and can include Brown-Séquard
syndrome, hemiparesis and quadriparesis, and
cruciate paralysis
77.
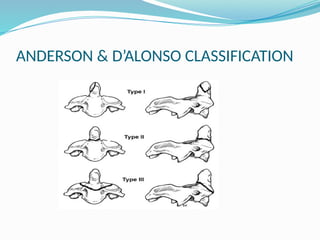
CLASSIFICATION
Type Iinjuries --oblique fractures to the upper
portion of the dens due to avulsion of the alar
ligament.
Type II dens fractures occur at the junction of
the dens with the central body of the axis,
lateral/ oblique force
In type III fractures the separation occurs in the
body of the axis and the fracture line primarily
involves cancellous bone.
ODONTOID #
TypeI- rigid immobilization in halo device
Type II- known for nonunion due to
displacement of fragments, Brooks & Jenkin’s
wiring or Gallie’s repair
Type III- Halo device
80.
HANGMAN’S #
Traumaticspondylolisthesis of C2
Second most common # of axis next to dens
# through pars interarticularis of axis seperating
neural arch from body of axis
Axial loading & hyper extension forces.
81.
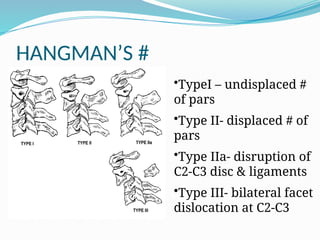
HANGMAN’S #
•TypeI –undisplaced #
of pars
•Type II- displaced # of
pars
•Type IIa- disruption of
C2-C3 disc & ligaments
•Type III- bilateral facet
dislocation at C2-C3
82.
TREATMENT
Type Ifractures as very stable and recommended
treatment in the cervical orthosis. The time period for
these fractures need not exceed 6 weeks of
immobilization.
Type II injuries of the arch of the axis are always
associated with some injury to either the anterior
longitudinal ligament, C2–C3 disk, or posterior
capsular structures.
The initial radiographic assessment is critical to
determining the direction of instability.
83.
Patients withtype II fractures should be
determined as to whether they are flexion-
extension or listhetic displacements and
attempts should be made through positioning
and traction to reduce the fractures.
Once reduction is achieved the patient is
placed into a halo vest and the fractures
reassessed radiographically.
If there is loss of fracture alignment, it can be
corrected by adjusting the halo. The patient
must wear the halo vest for at least 6 weeks.
84.
TREATMENT
Type IIa-Anterior C2- C3 stabilization with
arthrodesis
Type III- reduce with min traction, then posterior
C2- C3 arthrodesis.
85.
ALLEN CLASSIFICATION
Itis a mechanistic classification
Classified as 6 m.c pattern of c-spine injuries
1.flexion compression
2.vertical compression
3.flexion distraction
4.compressive extension
5.distractive extension
6.lateral flexion
Distraction Flexion
Mostcommon pattern
tensile failure and lengthening of post
column with possible compression of ant
column
ant.translation superior vertebra
25% facet subluxation
50% unilateral facet dislocation
> 50% bilateral dislocation
full body displacement
88.
Distractive flexion Injury
u/l facet dislocation
b/l facet dislocation
Postrerior ligamentous complex injury:
-manifested by widening of the interspinous
process space during flexion
-disruption of posterior ligamentous complex
may cause u/l or b/l facet dislocation
Treatment:
-healing is unlikely with external immobilization
-posterior cervical fusion with inter spinous
process wiring /oblique facet joint wiring
89.
Lateral Flexion Injuries
Unilateral fracture of the occipital condyle
Lateral mass of C1
Eccentric fracture of the superior articular
process of C2
Combination of the above mentioned injuries
90.
Extension Injuries
▪ Hyperextensionsprain dislocation
▪ Hyperextension fracture dislocation
▪ Laminar fracture
▪ Hangman fracture
▪ Extension teardrop fracture
▪ Avulsion horizontal fracture, anterior arch of
C1
▪ Fracture of the posterior arch of C1 (posterior
neural arch fracture of C1)
▪ Posterior atlantoaxial dislocation
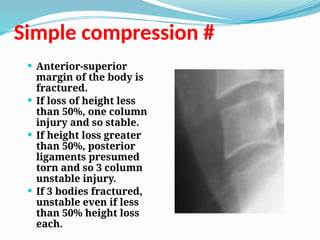
Anterior-superior
margin ofthe body is
fractured.
If loss of height less
than 50%, one column
injury and so stable.
If height loss greater
than 50%, posterior
ligaments presumed
torn and so 3 column
unstable injury.
If 3 bodies fractured,
unstable even if less
than 50% height loss
each.
Simple compression #
94.
Burst fractures
• Fractureof C3-C7 from
axial loadinng
• Spinal cord injury is
common from posterior
displacement of
fragments
• # is Stable if ligaments
intact
On lateral , body is
compressed anteriorly,
inferior end plate often
fractured, posterior body
contour is convex.
On AP, body fracture is
vertical or oblique and
95.
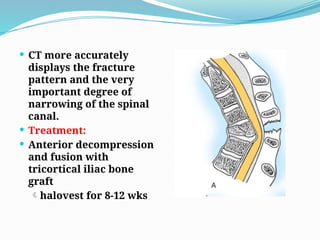
CT moreaccurately
displays the fracture
pattern and the very
important degree of
narrowing of the spinal
canal.
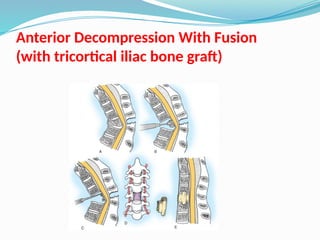
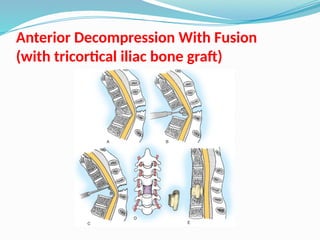
Treatment:
Anterior decompression
and fusion with
tricortical iliac bone
graft
halovest for 8-12 wks
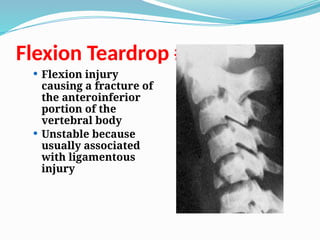
Flexion Teardrop #
Flexion injury
causing a fracture of
the anteroinferior
portion of the
vertebral body
Unstable because
usually associated
with ligamentous
injury
98.
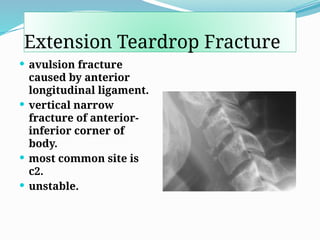
Extension Teardrop Fracture
avulsion fracture
caused by anterior
longitudinal ligament.
vertical narrow
fracture of anterior-
inferior corner of
body.
most common site is
c2.
unstable.
99.
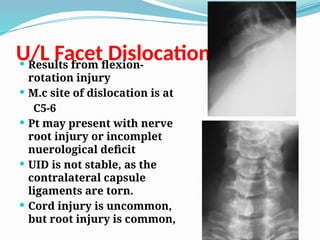
U/L Facet Dislocation
Results from flexion-
rotation injury
M.c site of dislocation is at
C5-6
Pt may present with nerve
root injury or incomplet
nuerological deficit
UID is not stable, as the
contralateral capsule
ligaments are torn.
Cord injury is uncommon,
but root injury is common,
100.
Treatment:
Reduction isdifficult with skeletal traction
Closed reduction may attemted to unlock (50%)
if reduced halovest immonbilization for
3months (stability would be obtained by
spontaneous fusion )
Open reduction internal fixation
Open redution and posterior cervical fusion
either with triple wiring or oblique facet
wiring, post operative rigid cervical arthrosios
for 6-8 wks
101.
Bilateral Facet Dislocation
Flexion rotation injury
also called “locked facets”
Subluxation of dislocated vertebra of
greater than ½ the AP diameter of the
vertebral body below it
High incidence of spinal cord injury (2/3)
- It is a severe 3 column injury that is
completely unstable.
Treatment:
Some heal with spontaneous interbody
fusion (unpredictable)
Closed traction reduction is associated with
increased risk of anterior disc herniation
-ORIF with interspinous wiring -(bohlman
triple wiring
oblique wiring-(inf.facet upper level spinous
process of lower level)
-
102.
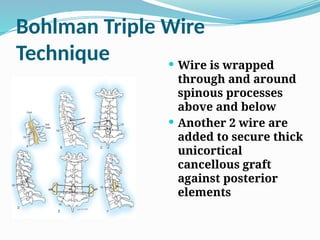
Bohlman Triple Wire
Technique Wire is wrapped
through and around
spinous processes
above and below
Another 2 wire are
added to secure thick
unicortical
cancellous graft
against posterior
elements
103.
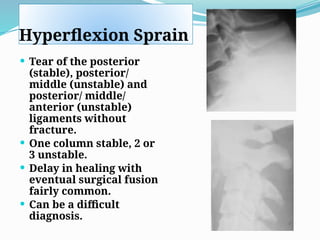
Hyperflexion Sprain
Tearof the posterior
(stable), posterior/
middle (unstable) and
posterior/ middle/
anterior (unstable)
ligaments without
fracture.
One column stable, 2 or
3 unstable.
Delay in healing with
eventual surgical fusion
fairly common.
Can be a difficult
diagnosis.
104.
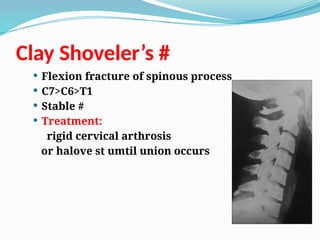
Clay Shoveler’s #
Flexion fracture of spinous process
C7>C6>T1
Stable #
Treatment:
rigid cervical arthrosis
or halove st umtil union occurs
105.
SCIWORA
Spinal CordInjury With Out Radiographic Abnormolity
12% spinal cord injury
DEFINITION
“Objective Signs Of Myelopathy As A Result Of Trauma With No
Evidence Of Fracture Or Ligamentous Instability On Plain X-ray And
Tomography”
Spinal cord is vulnerable to injury with out vertebral colomn
disruption
Occur predominantly in children
Because of inherent elasticity,Children have vertebrae that
can dislocate and quickly relocate. Cord gets damaged but
shows an aligned vertebral column.
Cord can be transected or compressed.
106.
On MRIparenchymatous hemorrhage and
contusions has bad results
finding of fracture, subluxation, or abnormal
intersegmental motion at level of neurological
injury excludes sciwora as a diagnosis
experimentally,
osteo-cartilaginous structures in spinal column can
stretch 2 inches without disruption -- spinal cord
ruptures after 1/4 inch
anatomically, cervical spinal cord is relatively
tethered - spinal nerves, dural attachment to
foramen magnum, and brachial plexus
107.
DEFINITION OF INSTABILITY
The loss of the ability of spine under
physiological load to maintain the
relationships between vertebrae In such a
way that the spinal cord or roots are not
damaged or irritated and deformity or
paindoes not developed
108.
CAUSE OF INSTABILITY
Traumatic
Neoplastic
Infectious disease
Iatrogenic
Acute :- bone or ligamentous disruption
Chronic :- progressive deformity
109.
MOTION SEGMENT:
Twoadjacent vertebrae and intervening soft tissue
In lower cervical spine it is devided into
-Anterior elements
-Posterior elements
STABLE:
All the anterior elements and one posterior
element intact
All posterior elements and one anterior element
intact
UNSTABLE:
All the anterior or posterior elements are not
functional
110.
PANJABI AND WHITE-CHECKLISTFOR
DIAGNOSIS OF CLINIAL INSTABILITY OF
LOWER C-SPINE
ELEMENT POINT VALUE
Anterior Elements Destroyed Or 2
Unable To Function
Posterior Elements Destroted Or 2
Unable To Function
Relative Sagittal Plane Translation >3.5mm 2
Ralative Sagittal Plane Rotation >11 Deg 2
Positive Stretch Test 2
Medullary (Cord) Damage 2
Root Damage 1
Abnormal Disc Narrowing 1
Dangerous Loading Anticipated 1
111.
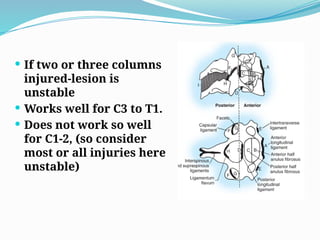
THREE COLUMN THEORYOF DENIS
ANTERIOR COLUMN -ALL
-Anterior half of the annulus fibrosus
-Anterior half of the vertebral body
MIDDLE COLUMN -PLL
-Posterior half of the annulus fibrosus
-Posterior half of the vertebral body
POSTERIOR COLUMN -inter transverse ligament
-Ligamentum flavum
-joint capsule
-Inter spinous ligament
-Supra spinous ligament
-Nueral arch
112.
If twoor three columns
injured-lesion is
unstable
Works well for C3 to T1.
Does not work so well
for C1-2, (so consider
most or all injuries here
unstable)
113.
GOALS OF TREATMENTOF C-SPINE
INJURIES
1. To realign the spine
2. To prevent loss of function of undamaged
nuerological tissue
3. To improve nuerological recovery
4. To obtain and maintain spinal stability
5. To obtain early functional recovery
114.
Pharmacological Management
Methylprednisolonesodium succinate (MPSS)
Within 3 hours 30mg/kg bolus + 5.4mg/kg/hr
infusion for 24 hours.
During 3~8 hours 30mg/kg bolus +
5.4mg/kg/hr infusion for 48 hours.
suppress inflammatory response and vasogenic
edema
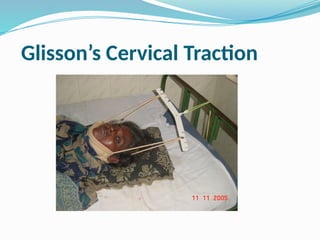
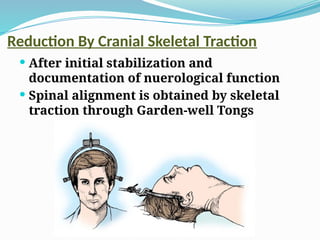
Reduction By CranialSkeletal Traction
After initial stabilization and
documentation of nuerological function
Spinal alignment is obtained by skeletal
traction through Garden-well Tongs
122.
Closed Reduction
Injuriesdemonstrating angulation, rotation or
shortening
restore normal alignment therefore decompressing
the spinal canal and enhancing neuro recovery
preventing further injury
need neuro monitoring and radiography
awake, alert and cooperative patient to provide
feedback
traction, positioning and weights ( 10 pds head and 5
pds each level below) xray after new weight applied
maintain after with 10-15 lbs traction
123.
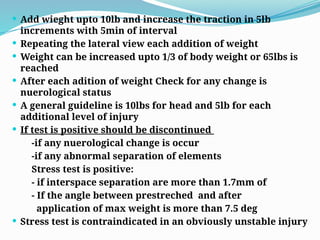
Add wieghtupto 10lb and increase the traction in 5lb
increments with 5min of interval
Repeating the lateral view each addition of weight
Weight can be increased upto 1/3 of body weight or 65lbs is
reached
After each adition of weight Check for any change is
nuerological status
A general guideline is 10lbs for head and 5lb for each
additional level of injury
If test is positive should be discontinued
-if any nuerological change is occur
-if any abnormal separation of elements
Stress test is positive:
- if interspace separation are more than 1.7mm of
- If the angle between prestreched and after
application of max weight is more than 7.5 deg
Stress test is contraindicated in an obviously unstable injury
124.
If spinalrealignment is abtained with traction
and is documented radiographically,weight is
reduced to 50% to maintain alignment to
prevent traction on vessels
If alignment cannot be obtained open
reduction and stabilization is usually by
posterior approach
125.
Non Operative Management
For stable c-spine injury with no compression of
neural elements
Immobilization in a rigid cervical orthrosis for 8-
12 wks
-Rigid cervical brace
-halovest
Evaluated by serial radiograph -weekly for 3
months,Then at 6wks,3 months,6months,1yr
Second complete evaluation should be performed
with in 3wks of injury to ruleout/evaluate
SUBACUTE INSTABILITY
126.
Surgical Decompression
Cervical spinalcord injury----
• During complete injury, no neurological
improvement in early or later decompression.
• During incomplete injury, controversial in
surgical decompression.
• Laminectomy may result in neurological
deterioration.
• Anterior cervical decompression may improve
function in incomplete quadriplegics
127.
• Experimental models--rapid decompression
better than later intervention.
• Human model— early reduction within 8 hours
brings significant recovery in one study;
however, some others against it.
• Increased risk such as pulmonary morbidity
associates early surgery.
128.
• Anterior approachis favoured;
• posterior laminectomy has no benefit and
worse cord compression.
• the only accepted indication for emergent
surgical treatment is progressive neurological
deterioration--- such as fracture displacement,
epidural hematoma, spinal cord edema or
infarction.
129.
Middle andlower cervical spine m.c exposed
through anterior approach
Anterior decompression and placement of
strut graft is safe and effective without
internal fixation
If posterior elements are stable addition of
anterior plate fixation to structural bone
grafting reduces motion at that level
130.
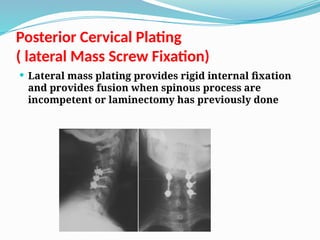
Posterior Cervical Plating
(lateral Mass Screw Fixation)
Lateral mass plating provides rigid internal fixation
and provides fusion when spinous process are
incompetent or laminectomy has previously done
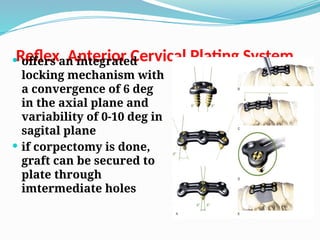
Reflex Anterior CervicalPlating System
offers an integrated
locking mechanism with
a convergence of 6 deg
in the axial plane and
variability of 0-10 deg in
sagital plane
if corpectomy is done,
graft can be secured to
plate through
imtermediate holes
134.
TAKE HOME MESSAGE
If have high enough index of suspicion to get x-rays,
then do not accept inadequate one
know your pediatric anatomical variations
do not forget nonskeletal injuries:
-ligamentous instability and
-sciwora
If a spinal fracture is identified at any level, the entire
spine should be examined with antero-posterior and lateral
views to document the presence or absence of spinal
fractures at other levels
don’t be in a hurry to clear the cervical spine - always leave
in a hard collar
Progressive neurological deficit in cord compression needs
early surgical decompression.
Anterior decompression is better.
Early surgical intervention for instability prevents
deterioration

![ANATOMY OF CERVICAL SPINE
Typical vertebrae [ C3- C6 ]
Atypical vertebrae
Atlas
Axis
C 7](https://image.slidesharecdn.com/newcspineinjuriesmyppt-250325140104-3894bc00/85/c-spine-injuries-classification-management-2-320.jpg)


![C1- C2 DISLOCATION
A] Forward dislocation with trans lig rupture
B] Forward subluxation with odontoid #
C] Posterior dislocation of atlas
D] Rotary subluxation](https://image.slidesharecdn.com/newcspineinjuriesmyppt-250325140104-3894bc00/85/c-spine-injuries-classification-management-74-320.jpg)