Downloaded 126 times
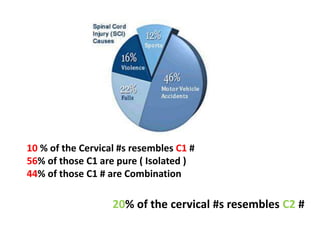


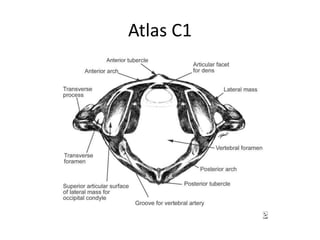
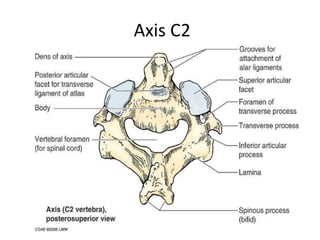
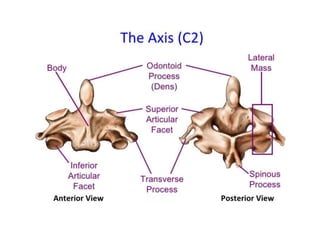
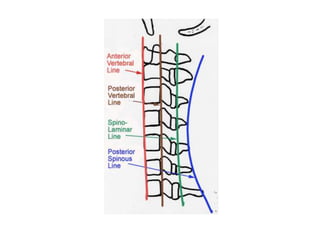


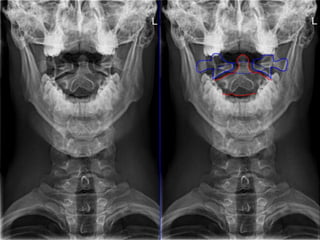
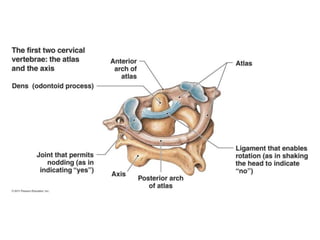
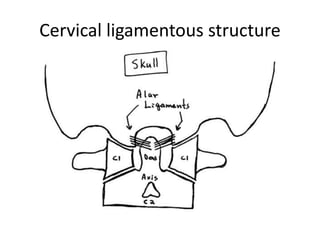
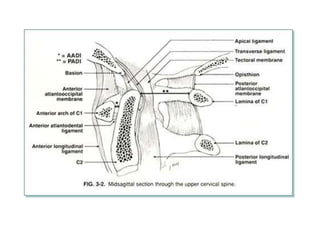
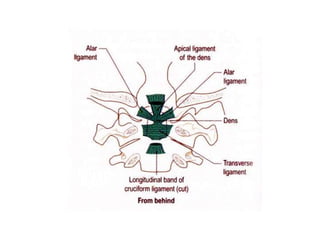

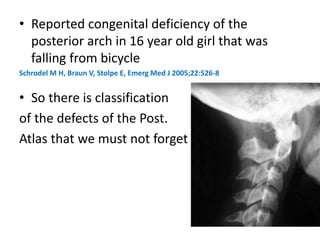
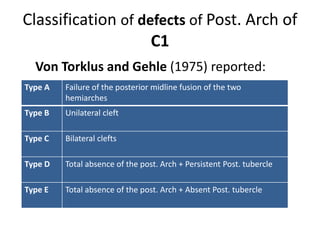
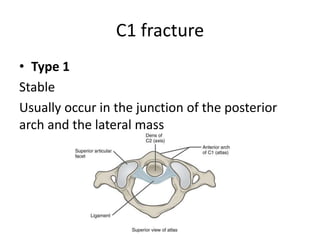
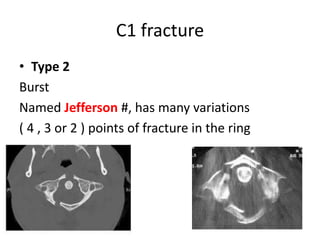
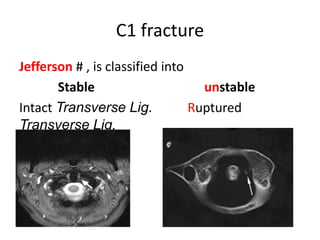
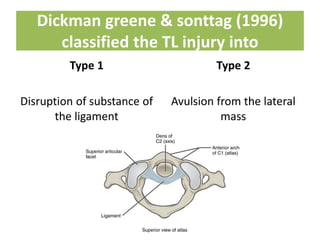
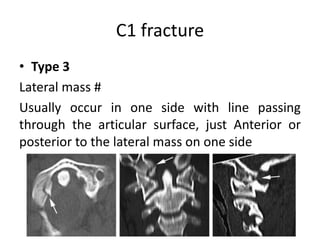
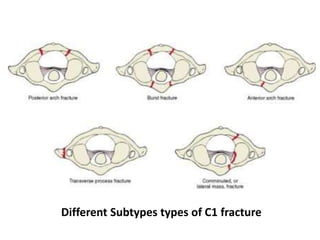
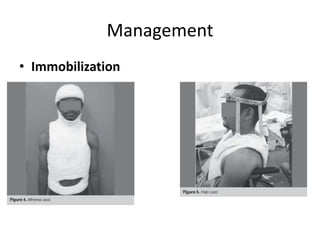

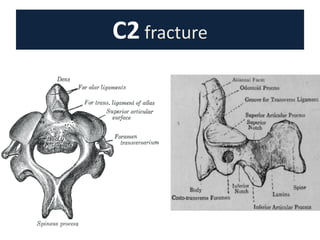
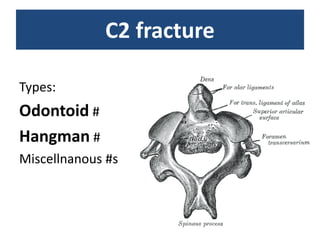
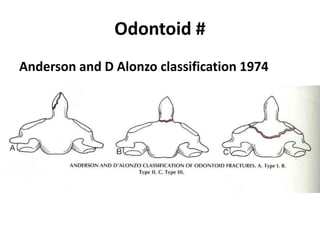
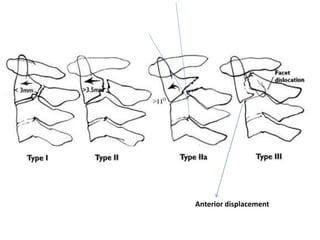
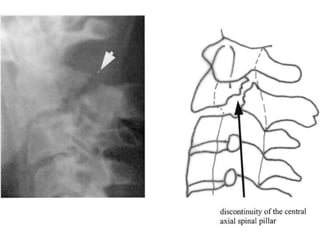
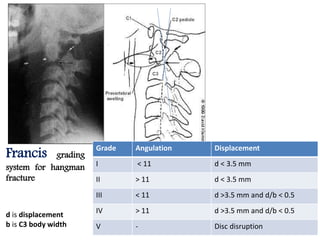
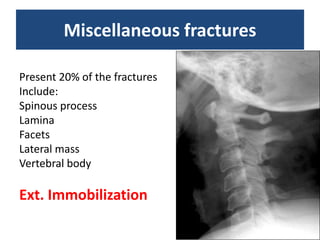
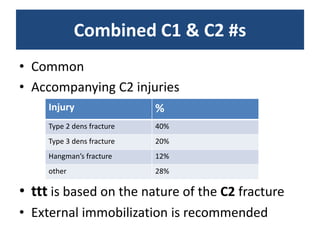
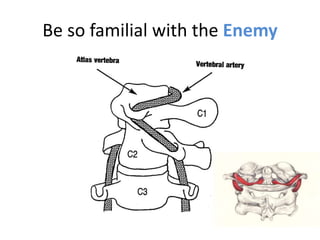





Cervical spine fractures, especially those involving C1 and C2, were discussed. Key points included that 10% of cervical fractures involve C1, with 56% being isolated fractures and 44% combined fractures. 20% involve C2. Types of C1 fractures described were Type 1 stable fractures at the posterior arch-lateral mass junction, Type 2 burst fractures, and Type 3 lateral mass fractures. Types of C2 fractures included odontoid fractures classified using Anderson and D'Alonzo's system, Hangman's fractures classified using Levine or Francis systems, and other miscellaneous fractures. Management depended on fracture type but often involved external immobilization though surgery may be indicated for unstable fractures or those with displacement,























































































