Downloaded 34 times




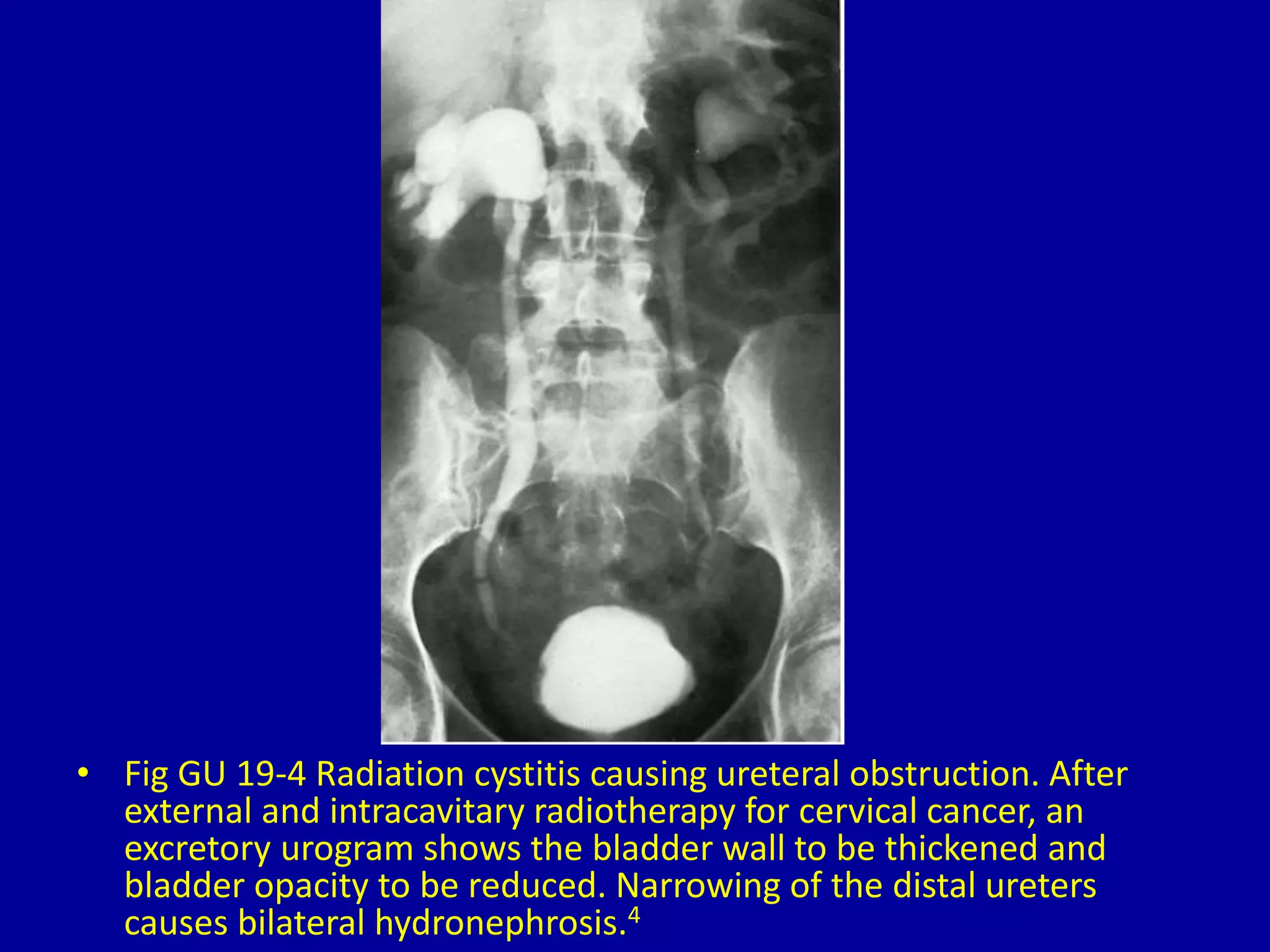
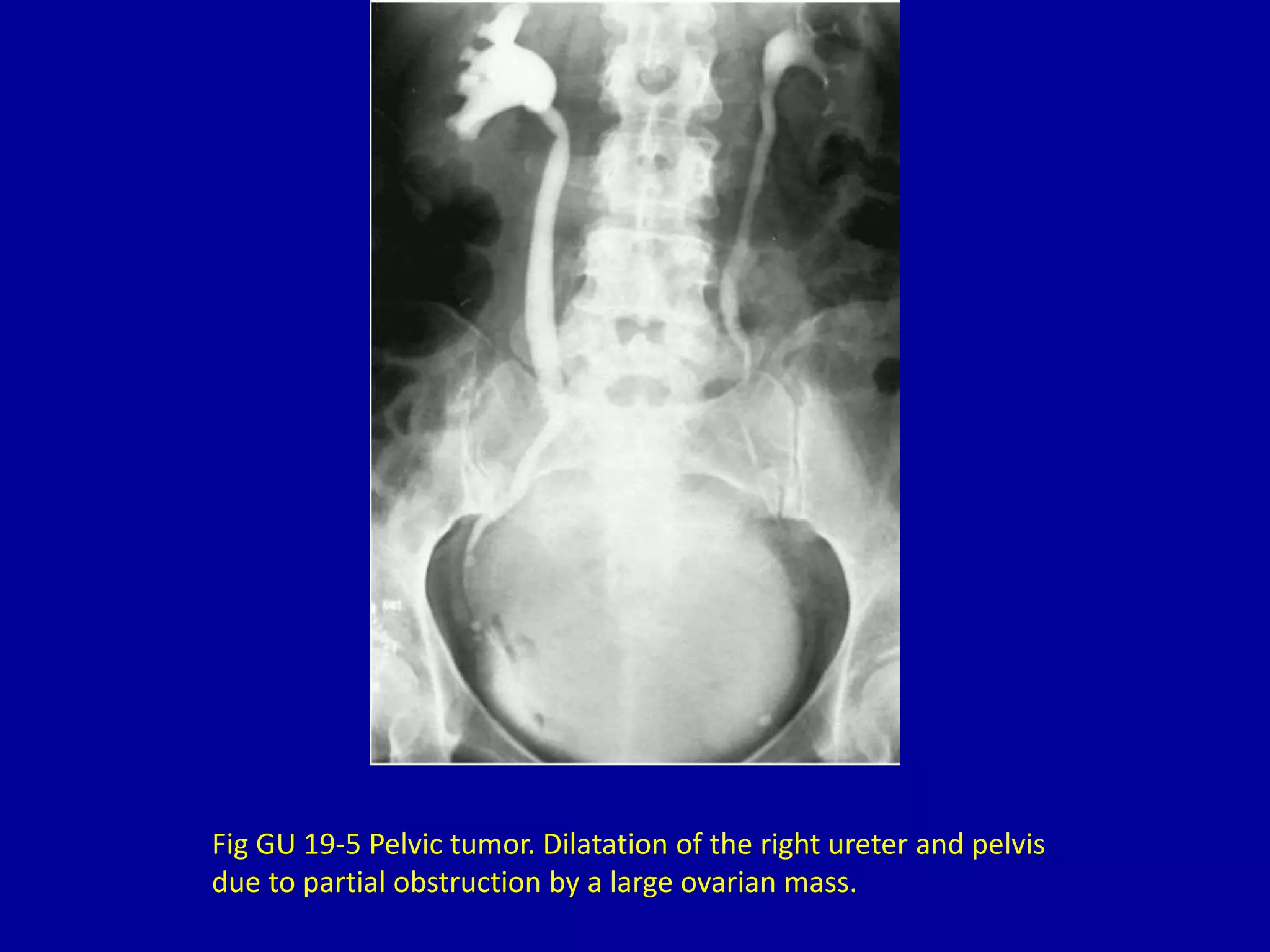


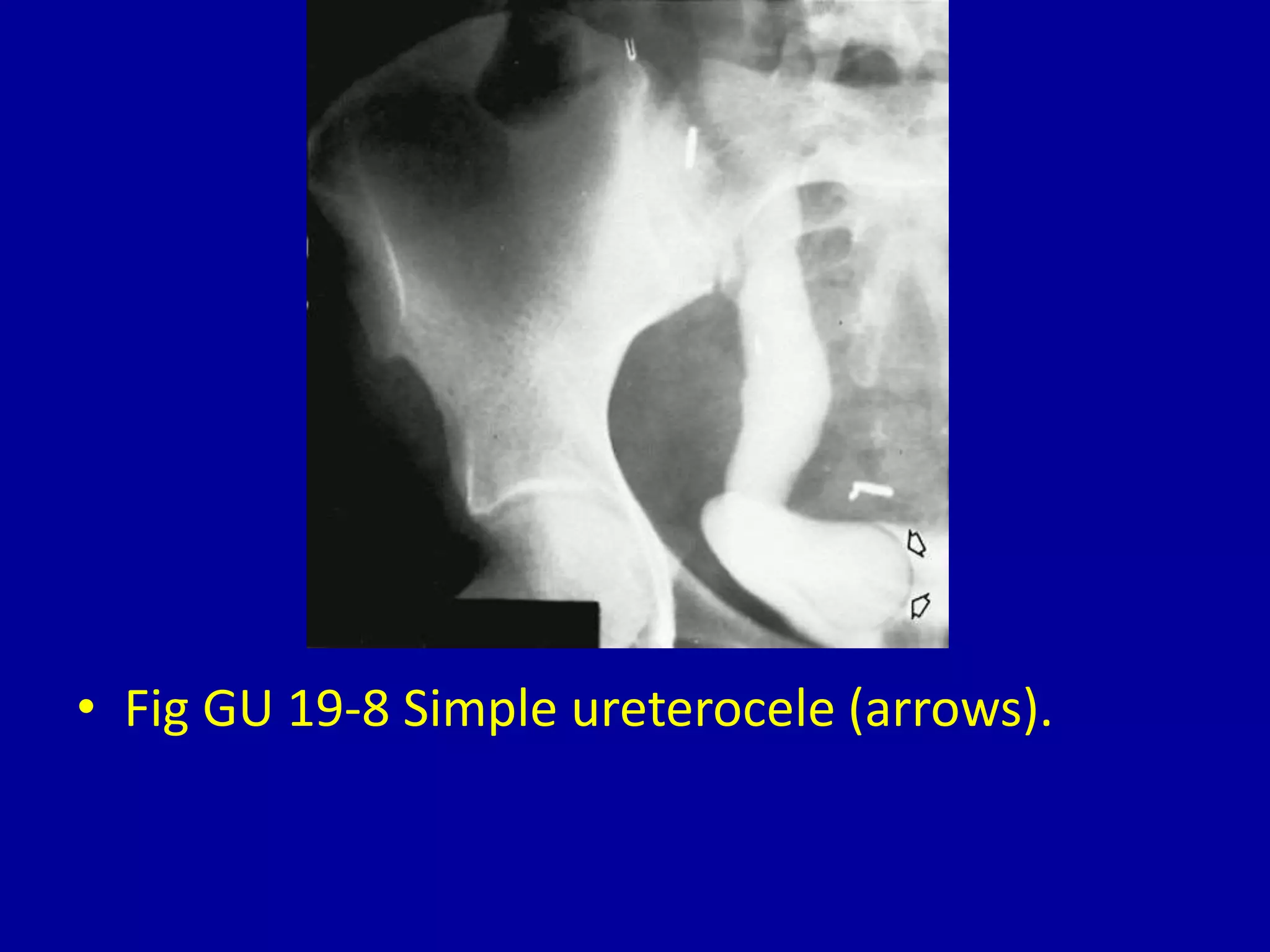
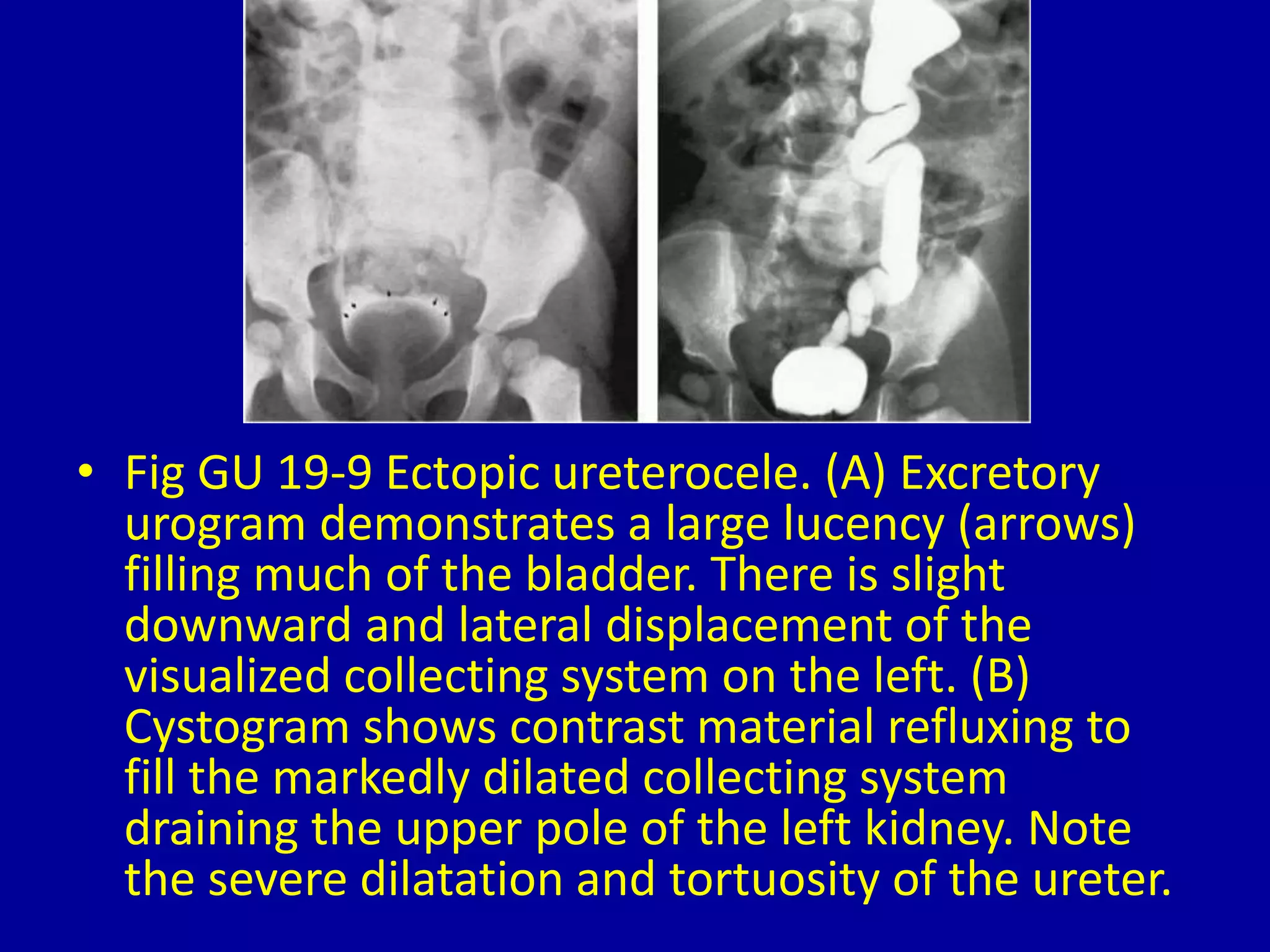

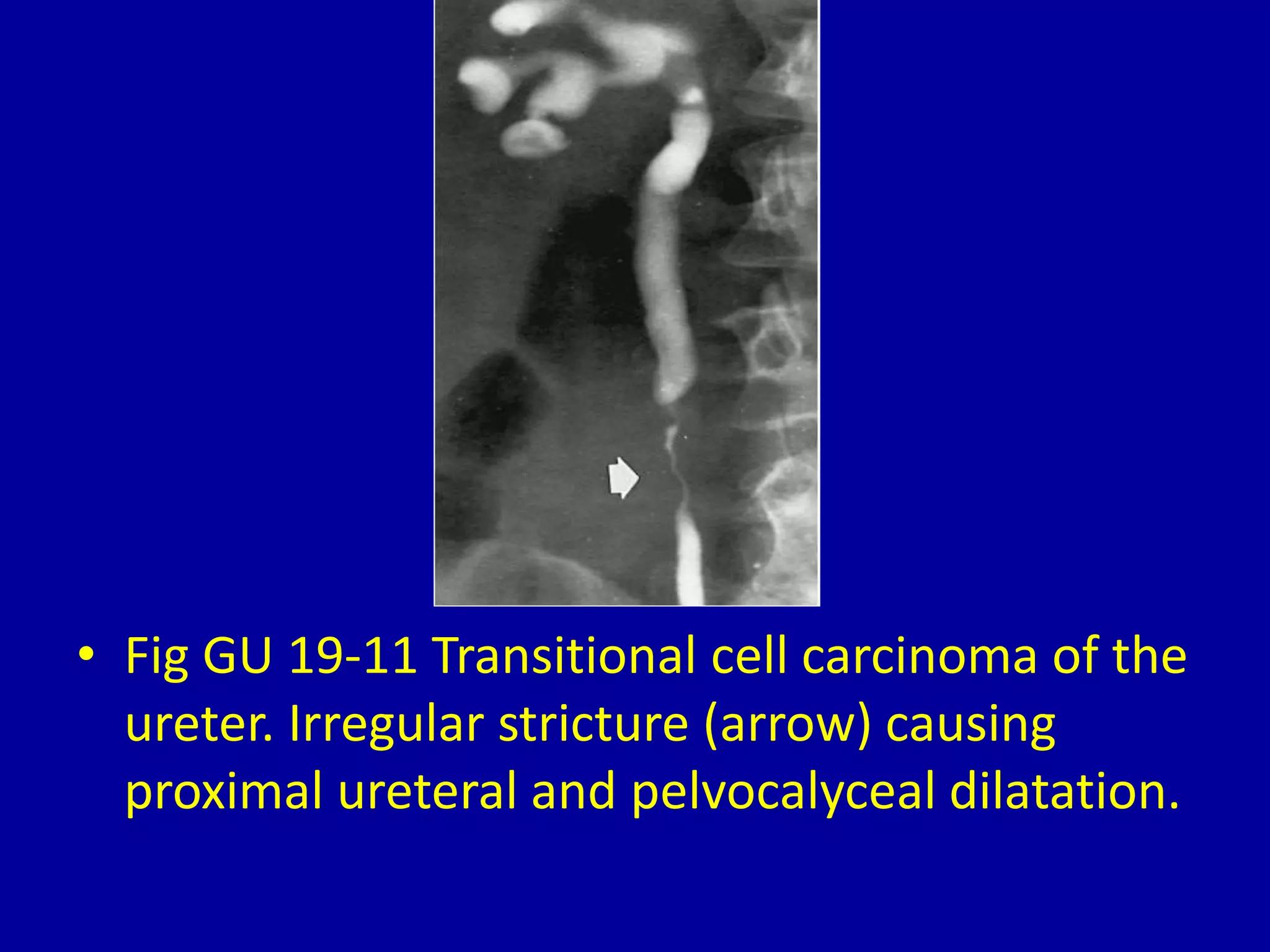

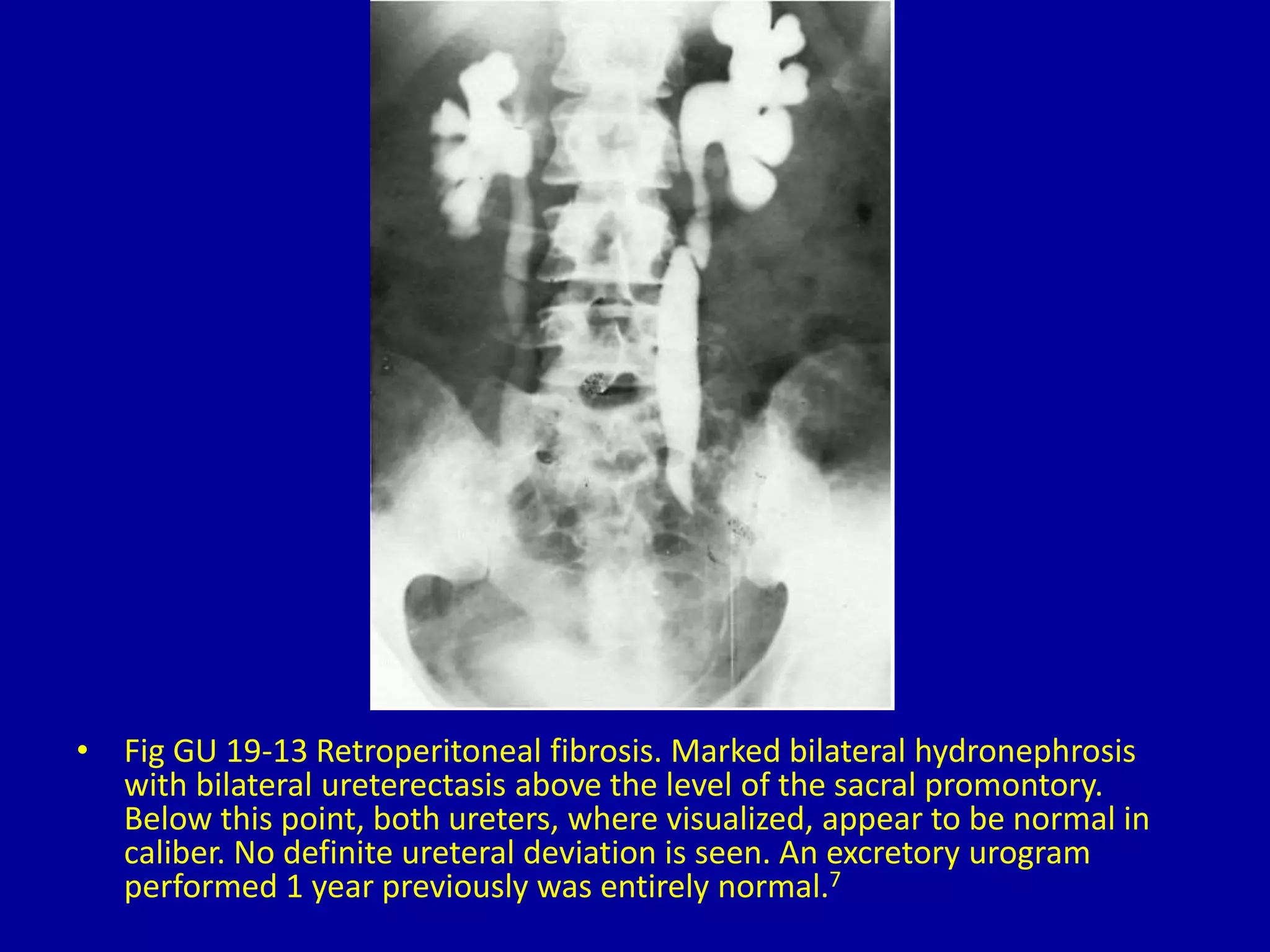





This document discusses and provides images of various causes of ureter obstruction, including kidney stones, congenital abnormalities, post-surgery strictures, radiation cystitis, pelvic tumors, bladder cancer, interstitial cystitis, ureteroceles, retrocaval ureters, transitional cell carcinoma, hydronephrosis of pregnancy, retroperitoneal fibrosis, and obstructing valves at the ureteropelvic junction. The images demonstrate dilated ureters and kidneys caused by proximal obstructions from these various etiologies.











































































































