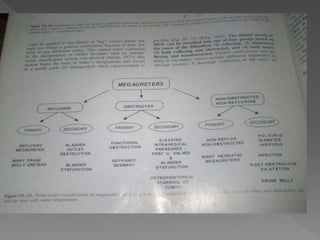
- Megaureter (MGU) is defined as a ureteral diameter greater than 7 mm. MGU can be classified based on its cause as refluxing, obstructed, both refluxing and obstructed, or nonrefluxing and nonobstructed.
- MGU is a common finding in neonates referred for urologic evaluation and accounts for up to 23% of cases of urinary tract dilatation seen on prenatal ultrasound.
- Evaluation of MGU involves ultrasound to assess anatomy and severity, VCUG to check for reflux, renal scan to evaluate function, and potentially MRI urography.
- Management depends on etiology but