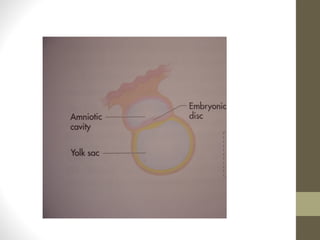
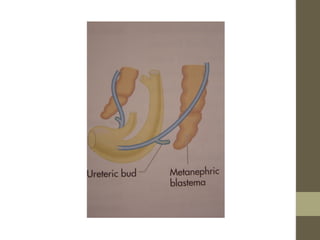
The document provides an overview of urinary tract anatomy and relevant pathologies. It begins with basic embryology of the urinary tract including the development of the kidneys, ureters, and bladder from the intermediate mesoderm. Key anatomical landmarks of the kidneys and ureters are described. Examples of pathologies discussed include duplex renal systems which can cause upper pole obstruction and hydronephrosis. PUJ obstruction is explained as a restriction of flow from the renal pelvis to ureter that can lead to renal deterioration if left untreated. Renal calculi cause pain when they obstruct the urinary tract at various positions from the infundibulum to the VUJ.








































![Emergency in Urology [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/emergencyuroedmond-140716213857-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


































































