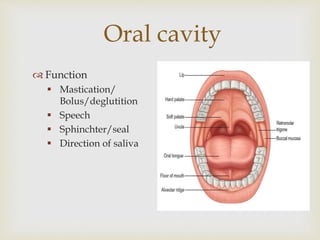
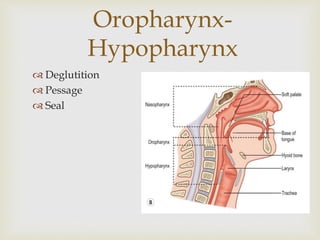
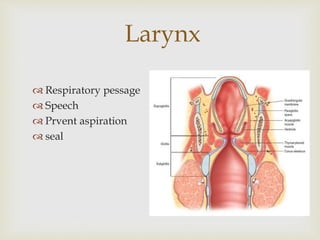
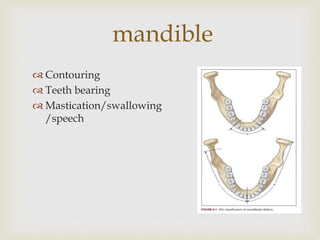
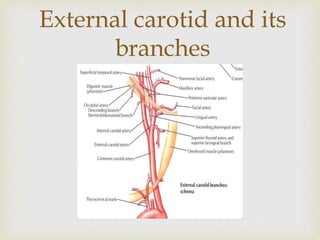
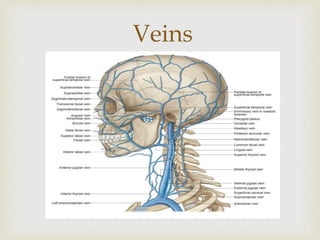



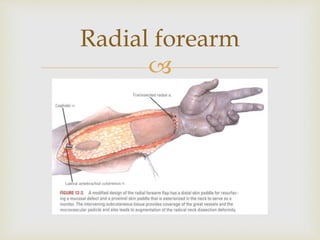
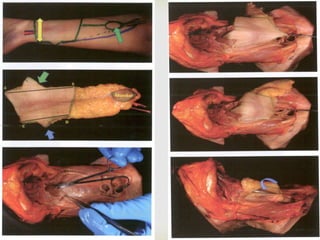
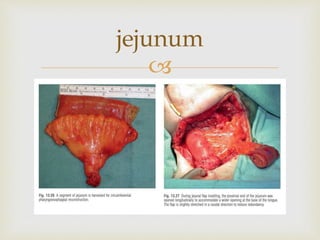
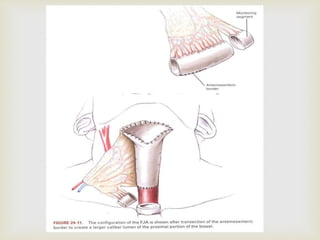




This document discusses head and neck cancer reconstruction using free flaps. It begins by outlining the anatomy of the head and neck region and factors to consider for reconstruction such as integrity, function and form. Common free flap options are described including the anterolateral thigh flap, radial forearm flap, rectus abdominis flap, fibula flap and jejunum flap. Key steps in planning a reconstruction including evaluating the defect, donor site, patient factors and surgical experience are highlighted. The importance of microvascular expertise and equipment for free flap reconstruction is emphasized.



































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)

















