Downloaded 48 times
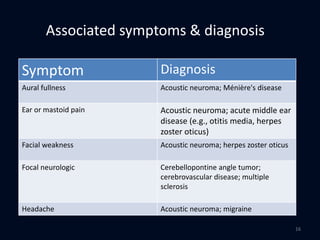
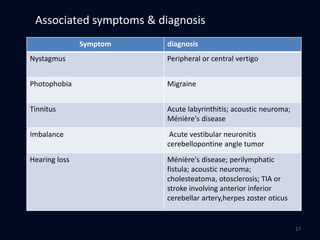
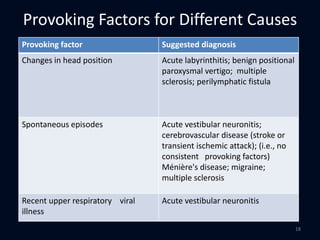
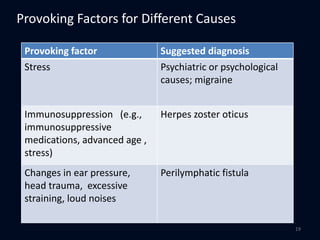
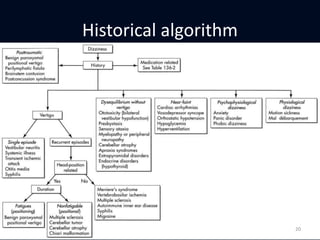

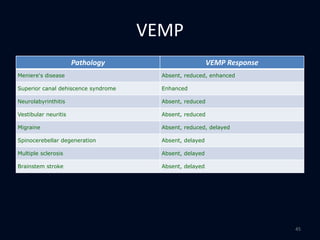

This document provides an overview of evaluating patients presenting with dizziness or vertigo. It discusses classifying vertigo based on duration, whether it is central or peripheral in origin, and non-vestibular causes. A thorough history and physical exam including neurologic and vestibular testing is outlined. Key diagnostic tests like Dix-Hallpike, caloric testing, and VEMP are described. Common causes of vertigo like BPPV, vestibular neuronitis, and Meniere's disease are highlighted based on presenting symptoms, exam findings, and test results.





















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

