Downloaded 305 times
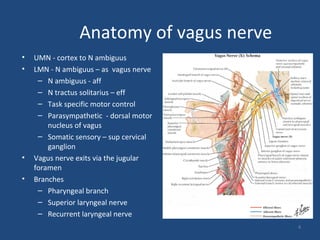
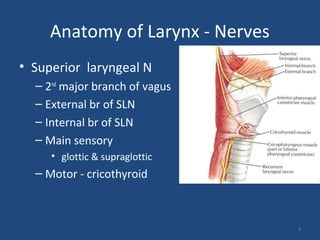
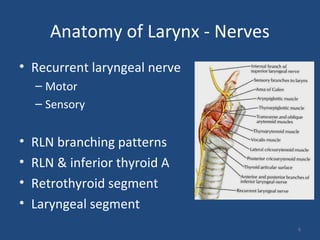
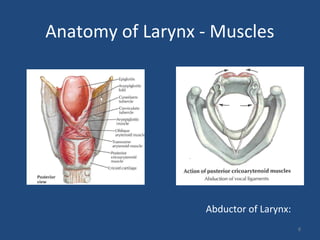
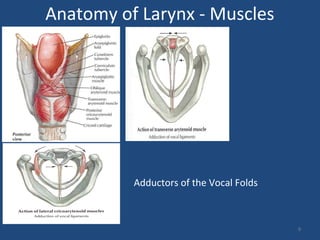
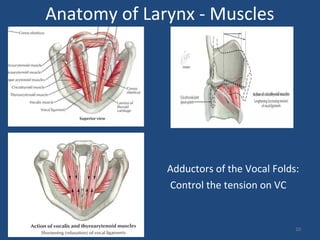
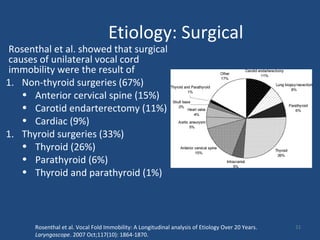






This document provides information on vocal cord paralysis, including: 1. It summarizes the anatomy of the larynx, nerves, and muscles as well as the functions of the larynx. 2. It discusses the various causes (etiologies) of vocal cord paralysis including surgical, malignant, inflammatory, traumatic, neurological and others. 3. It describes the clinical assessment and evaluation of a patient with vocal cord paralysis including history, examination findings, and surgical evaluation techniques.























































































