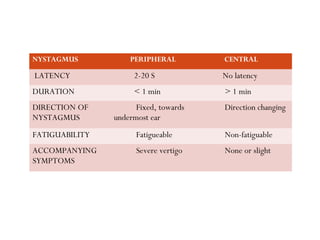
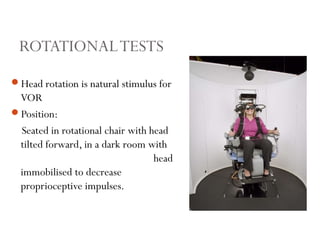
This document discusses the evaluation and management of patients presenting with vertigo. It begins with definitions of types of dizziness including vertigo, lightheadedness, presyncope, disequilibrium, and oscillopsia. It then covers the causes of vertigo which can be peripheral involving the vestibular end organs or central involving the brainstem or cerebellum. The document outlines the history, examination including vestibular function tests like caloric testing and rotational chair, and interpretation of results for diagnosing the cause and site of lesion for vertigo.