Download as PDF, PPTX


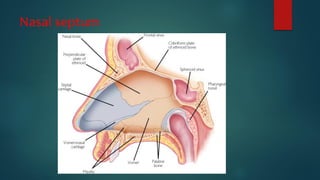
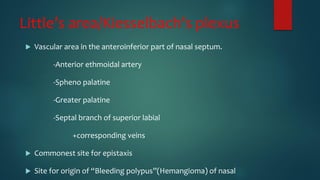
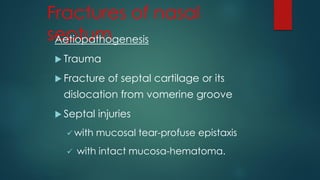
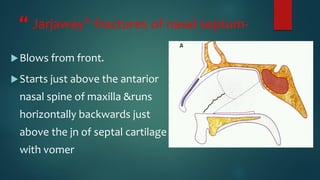
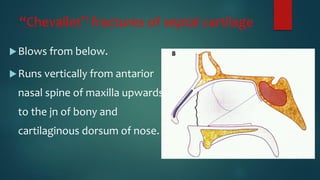
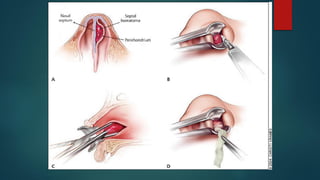
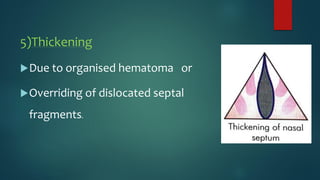

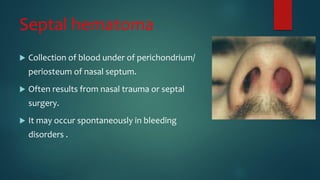



The nasal septum has 3 parts - the columellar septum, membranous septum, and septum proper. The septum proper provides structural support to the nose and is formed by bones and cartilage. The nasal septum is supplied by blood vessels and nerves and is prone to fractures and deviations from trauma. Deviated septum and septal hematomas can cause nasal obstruction and other issues. Septal abscesses may develop from infections of hematomas and can destroy cartilage. Perforations can occur from trauma, infections, drugs, or idiopathic causes. Small perforations may cause whistling sounds while larger perforations require management of crusts.




























![Nasal septum and its diseases[1]](https://cdn.slidesharecdn.com/ss_thumbnails/nasalseptumanditsdiseases1-140421073429-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












