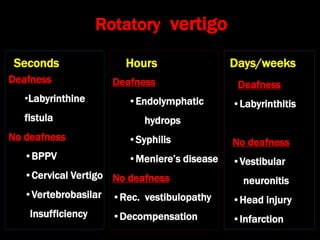
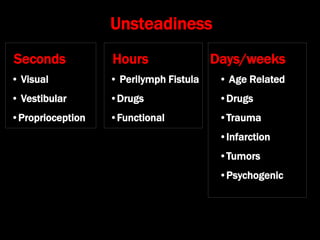
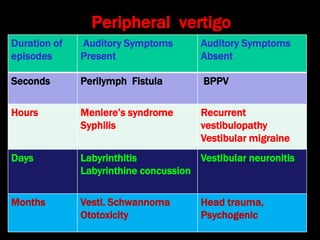
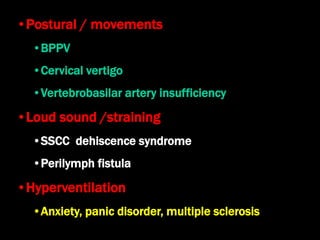
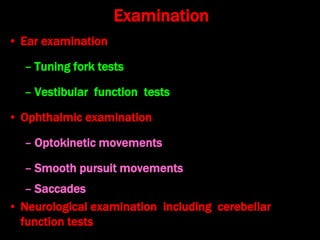
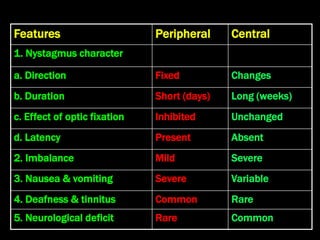
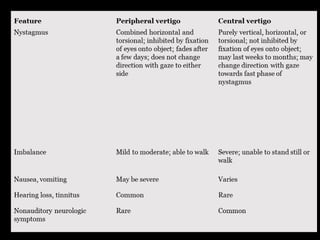
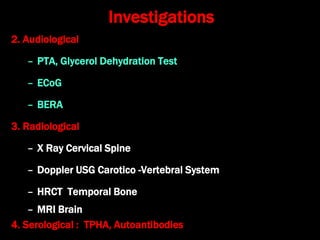
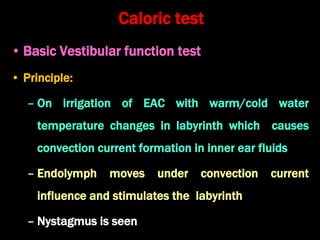
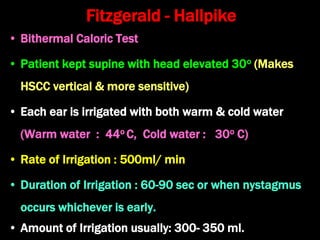
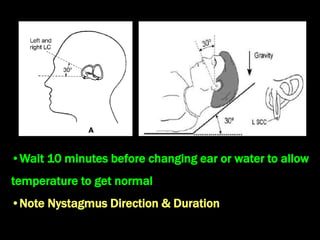
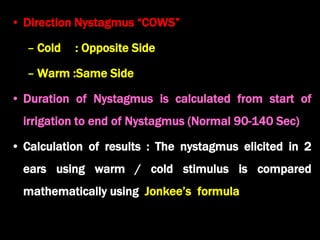
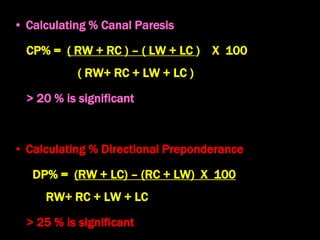
This document discusses the evaluation of vertigo. It defines vertigo and classifies it according to duration. It describes the characteristics of peripheral vertigo such as associated hearing loss, episodic nature, and association with head movement. The document outlines tests used to investigate peripheral vertigo, including the caloric test and Fitzgerald-Hallpike test, and how to differentiate between peripheral vertigo and central vertigo based on features like nystagmus characteristics and neurological deficits.

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






