Downloaded 120 times
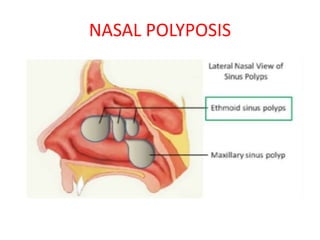
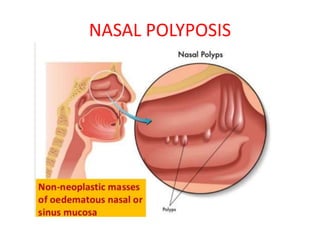
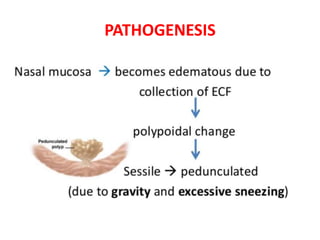
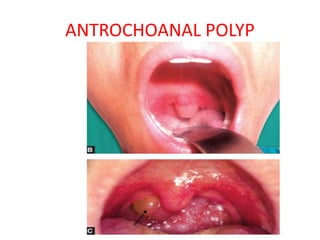
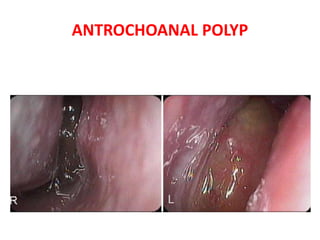

This document discusses nasal polyposis, including its definition, epidemiology, etiology, pathogenesis, pathology, symptoms, signs, diagnosis and treatment. Some key points include: - Nasal polyps are soft, non-cancerous growths that develop in the nasal cavity or sinuses. The two main types are ethmoidal polyps and antrochoanal polyps. - Ethmoidal polyps are more common in adults and often associated with chronic rhinosinusitis, asthma or allergies. Antrochoanal polyps usually present in adolescents and originate in the maxillary sinus. - Symptoms include nasal obstruction, loss of smell, discharge and headaches. Diagnosis involves























































































