Downloaded 600 times






















This document discusses abdominal abscesses, including: - Definitions and types of abdominal abscesses - Pathophysiology, factors that favor abscess formation, and clinical features - Diagnostic tests including X-ray, CT scan, USG, and MRI - Management including adequate resuscitation, antimicrobial therapy, and source control through percutaneous or surgical drainage - Specific discussions of pyogenic liver abscesses, amoebic liver abscesses, prerequisites and complications of percutaneous drainage, and criteria for drain removal
Presenter introductions with Dr. A R Shaan and Dr. S B Choudhary; Focus on Michael DeBakey and Alton Oschner.
Definition of abdominal abscess; Types include intraperitoneal, visceral, and retroperitoneal.
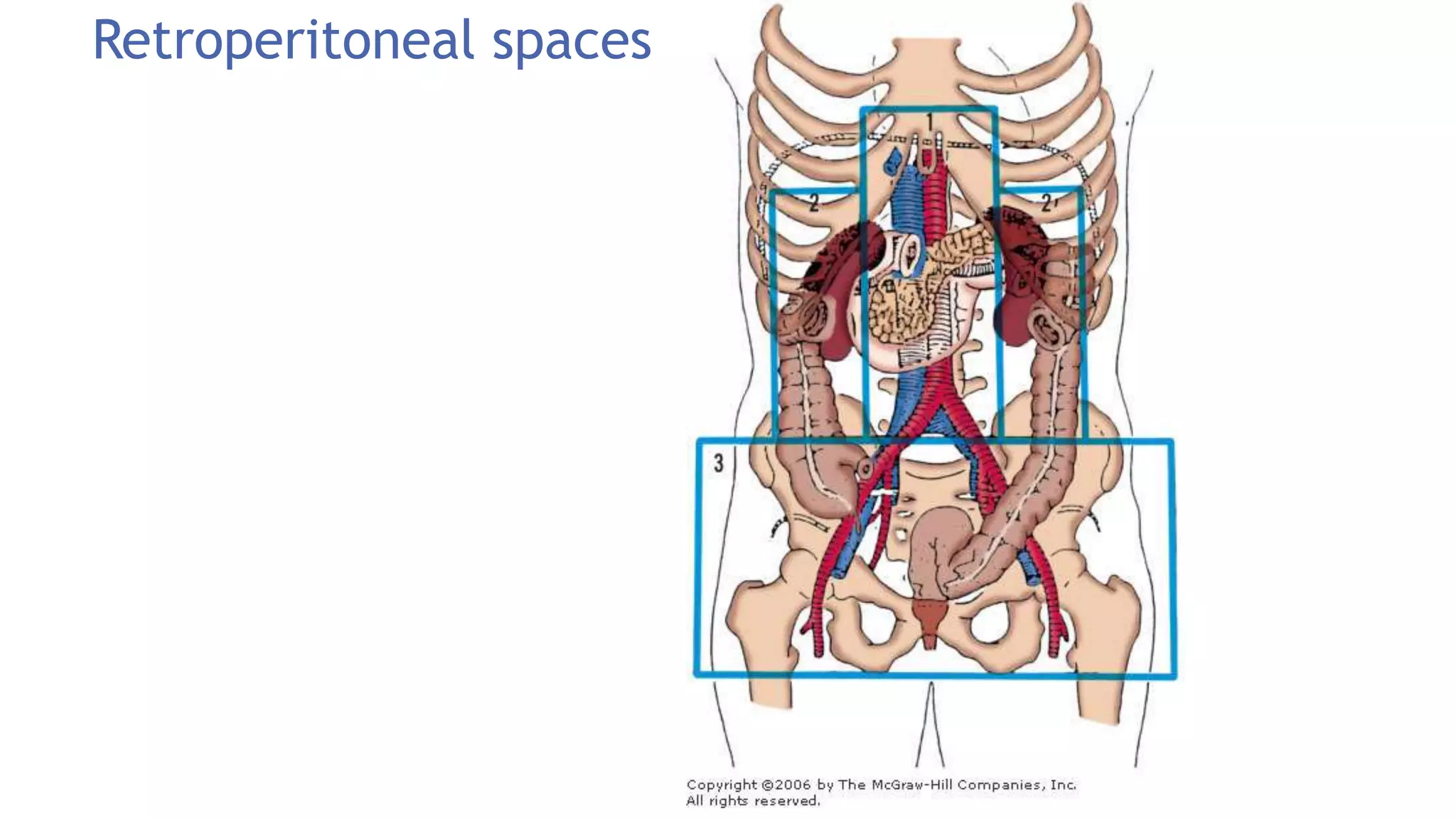
Overview of intraperitoneal and retroperitoneal spaces; Causes of extravisceral abscesses.
Defense mechanisms in the peritoneal cavity; Components involved include macrophages and cytokines.
Clinical symptoms like fever and localized pain; Highlights abscess types such as subphrenic.
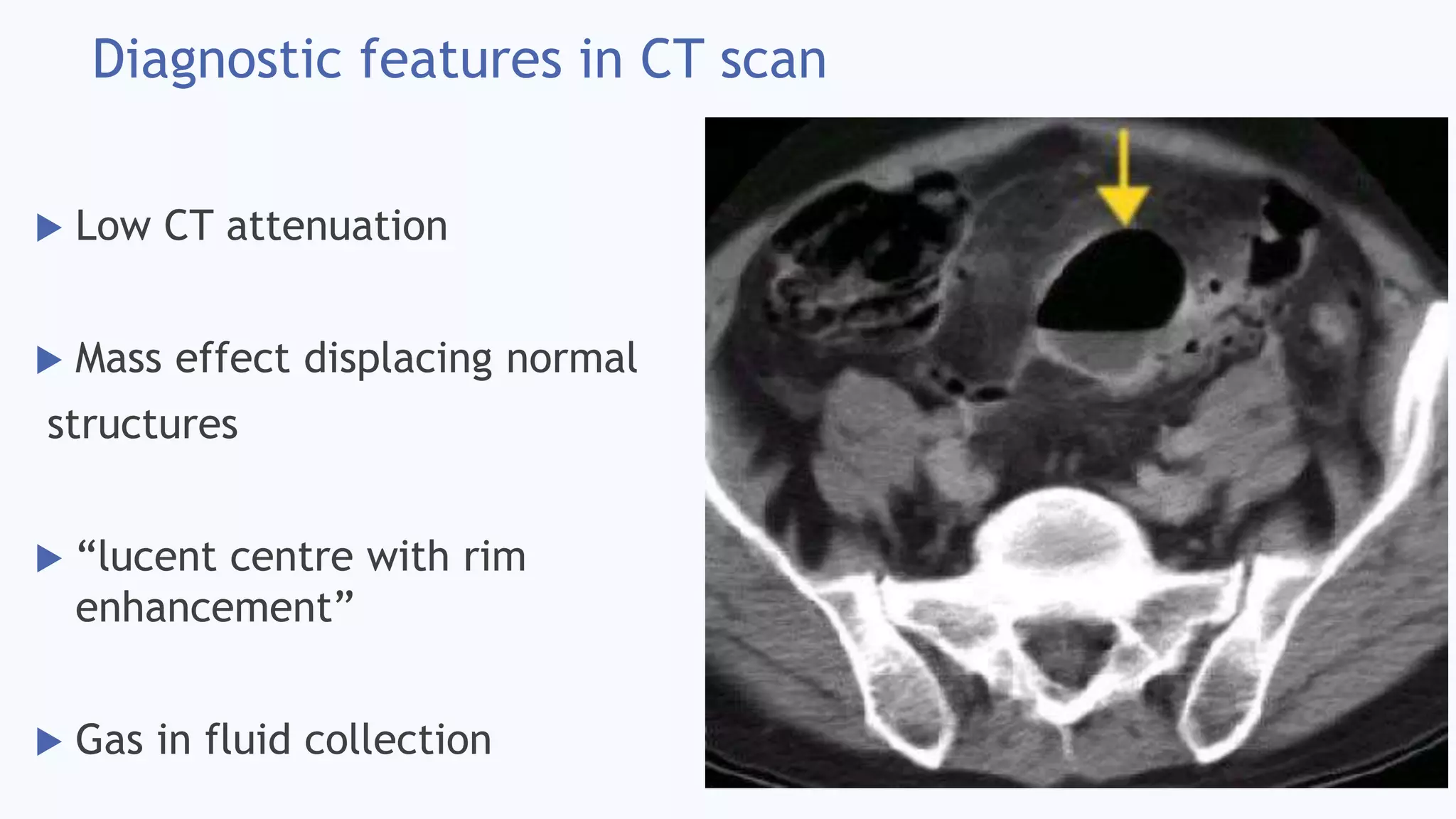
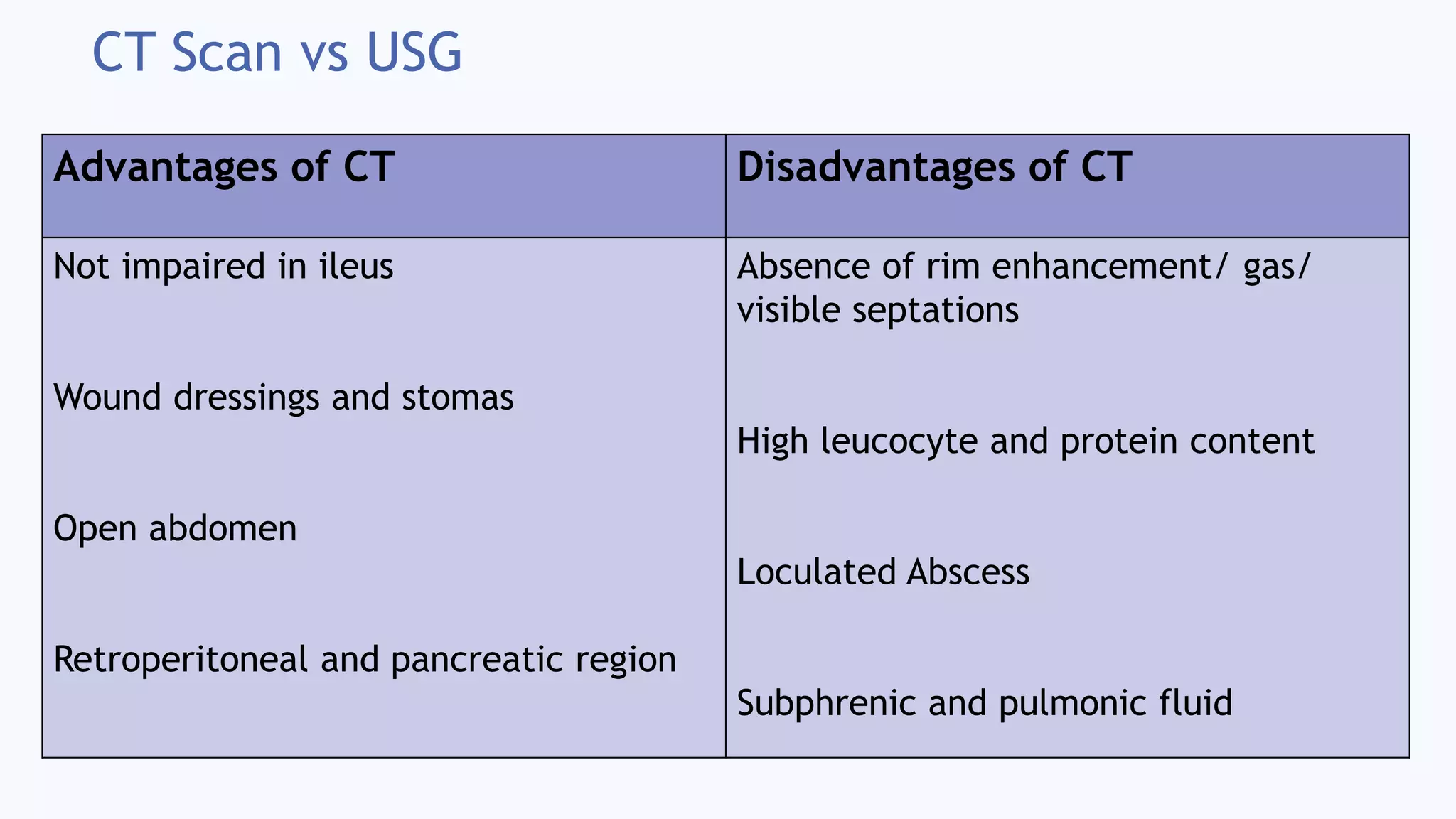
Diagnostic methods include imaging via X-ray, CT, and MRI; Key features of diagnostics.
Management includes resuscitation, antimicrobial therapy, and source control.
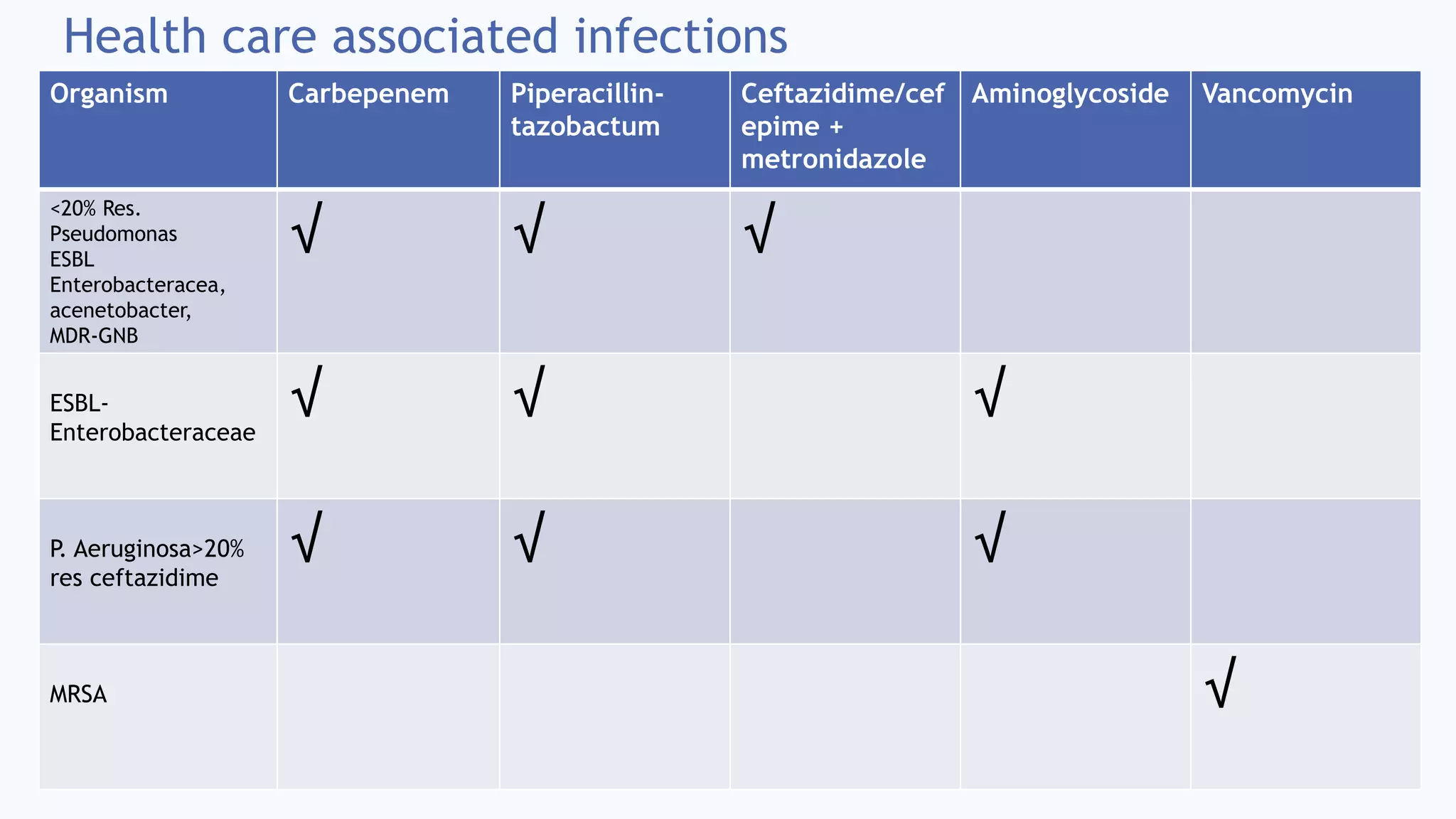
Categories of antimicrobial therapy for community and healthcare-associated infections.
Management for pyogenic and amoebic liver abscesses including antibiotic and drainage strategies.
Techniques for percutaneous drainage; prerequisites and post-requisites for successful outcomes.
Complications during drainage include sepsis; Guidelines for drain removal based on clinical parameters.
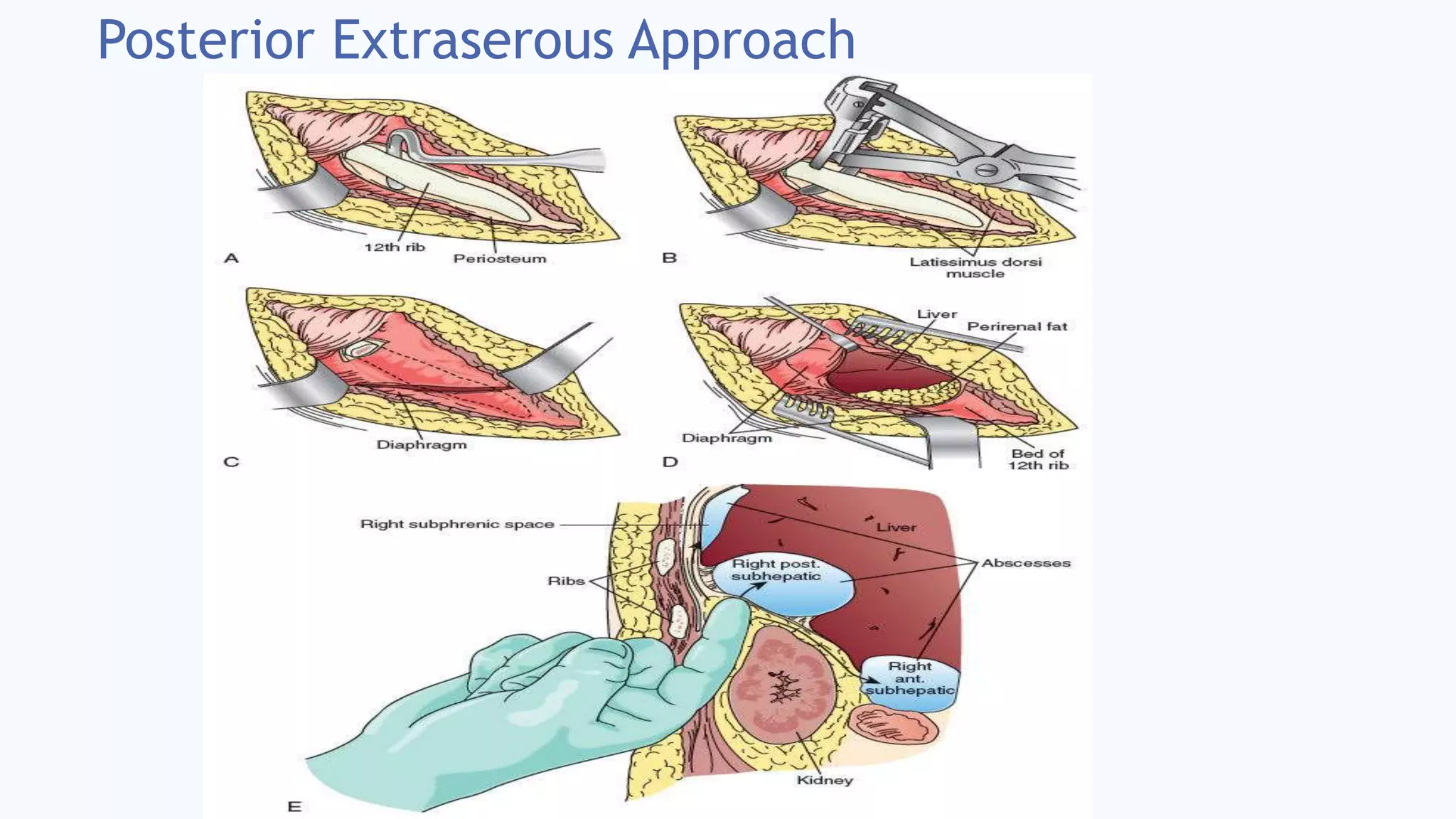
Surgical options for abscess management; Insights on transperitoneal and extraperitoneal approaches.
Quote by Berkeley Moynihan reflecting on surgery's experimental nature in bacteriology.





























































































