

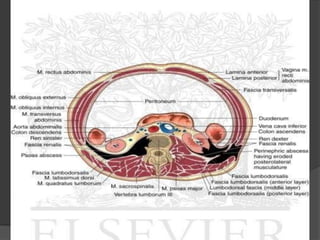


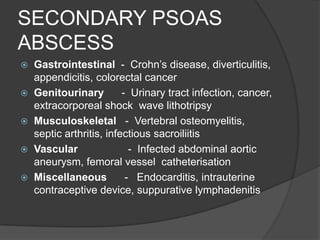


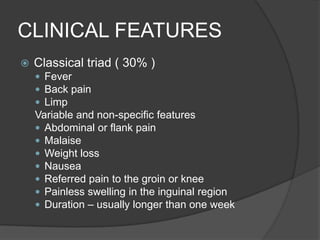
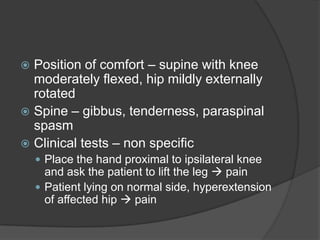












This document discusses psoas abscess, which is a collection of pus in the iliopsoas compartment. Psoas abscess can be primary (from hematogenous spread) or secondary (from infection of adjacent organs). Common causes of secondary psoas abscess include gastrointestinal, genitourinary, musculoskeletal, and vascular infections. Clinical features can include fever, back pain, limp, and abdominal or groin pain. Diagnosis involves blood tests and imaging like CT or MRI. Treatment requires appropriate antibiotics and drainage of the abscess, either percutaneously or through open drainage.



































































