The document discusses the clinical evaluation and management of intra-abdominal infections. It describes how the history, physical exam, blood tests and imaging can be used to evaluate the patient and determine the source and severity of infection. Depending on the findings, options for treatment may include antibiotics alone, percutaneous drainage of abscesses, or surgical intervention such as drainage or resection of infected tissues. The specific approach depends on the location and characteristics of the infection based on the diagnostic evaluation.
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 1
18 INTRA-ABDOMINAL INFECTION
Robert G. Sawyer, M.D., F.A.C.S., Jeffrey S. Barkun, M.D., F.A.C.S., Robert Smith, M.D.,T Chong, M.D., and George Tzimas, M.D.
ae
Recognition and Management of Intra-abdominal Infection
The basic principles of rapid diagnosis, timely physiologic sup- whereas a stable patient presenting with a chronic complaint can
port, and definitive intervention for intra-abdominal infections be evaluated in a more deliberate fashion.The specifics of the pre-
have remained unchanged over the past century. Specific manage- senting episode (e.g., the onset, location, and nature of the pain
ment of these conditions, however, has been transformed of late as and any changes in bowel habits) are undeniably crucial, but the
a result of numerous advances in technology. Improved radiologic patient’s medical and surgical histories, as well as any previous
and laboratory techniques have led to more precise preoperative similar illnesses, are equally critical. Many medical problems and
diagnoses, and newer procedures have led to treatment algorithms therapies are associated with abdominal pain or discomfort, and
that cause less morbidity and permit faster recovery. Whereas the an accurate accounting of previous surgical manipulation of the
pathophysiology of these infections remains largely unchanged, abdomen is vital for refining the differential diagnosis, as well as
their management is now marked by an ever-growing complexity. for prioritizing further tests.The question of whether a patient has
It is no longer true that the diagnosis of intra-abdominal infection, presented with similar symptoms before (particularly if those
even in association with a perforated viscus, necessitates urgent symptoms led to a diagnosis) may be important for determining
exploration, but it remains the case that decisions regarding the the timing of any intervention, as well as for putting the current
ultimate course of action for any individual patient are solely the complaint in the context of an ongoing condition. In fact, many
responsibility of the surgeon. patients arrive for medical treatment with a strong (and frequent-
ly correct) concept of the nature of their disease.
Clinical Evaluation PHYSICAL EXAMINATION
Once the history has been obtained, a thorough physical assess-
HISTORY
ment is performed, with the emphasis on the abdomen, the pelvis
The general approach to a patient sus- (including the vagina), and the rectum. The usual sequence—
pected of having an intra-abdominal inspection, auscultation, percussion, and palpation—should be
infection is much like that to a patient followed as traditionally taught.This sequence need not be exten-
with any other acute surgical condition. sively reviewed here; however, certain points should be empha-
Specific approaches to various intra- sized. With the advent of laparoscopy, inspection must include a
abdominal infections are addressed in more detail elsewhere [see careful search for scars indicating previous operations, given that
Infections of the Upper Abdomen and Infections of the Lower any laparoscopic procedure can be undertaken by way of a variety
Abdomen, below]. of trocar sites. Auscultation, though occasionally helpful, is also
The first step is an accurate history.To begin with, cases of peri- probably the least specific form of examination. Percussion is valu-
tonitis are broadly classified as primary, secondary, or tertiary; this able for assessing tenderness, as well as for differentiating abdom-
classification provides a useful framework for suggesting general inal distention caused by intraluminal gas or free air (signaled by
approaches to treatment. Primary peritonitis arises spontaneously, tympany) from that caused by fluid in the peritoneum, such as
without a demonstrable source of contamination, and is generally ascitic fluid or blood (signaled by dullness).
treated with antibiotics alone; an example is spontaneous bacteri- Proper and humane assessment of the abdomen for tenderness
al peritonitis in the setting of ascites. Secondary peritonitis is via palpation can be learned only through extensive experience.
caused by a breach in the GI tract that leads to contamination of Gaining the patient’s trust is fundamental: an anxious or dis-
a normally sterile space. Control of the source of infection via tressed examinee may respond in a hypersensitive manner, there-
drainage, resection, diversion, or some combination thereof is by hindering the acquisition of information. An individualized
imperative for optimizing outcome. Tertiary peritonitis is a poorly approach is essential as well. Palpation should not be performed in
defined entity associated with recurrence of intra-abdominal infec- a uniform manner from patient to patient; rather, the amount of
tion after the treatment of secondary peritonitis. It frequently fea- tenderness present ought to be judged by the degree of pressure
tures a diffuse infection in a critically ill patient and may be caused or indentation required to cause a given patient significant dis-
by any of a long list of nosocomial pathogens (e.g., Pseudomonas comfort. In the setting of severe abdominal pain, elicitation of
aeruginosa, Staphylococcus aureus, and Candida albicans). Manage- rebound tenderness by means of deep palpation followed by rapid
ment of tertiary peritonitis is complex and must be individualized release of pressure usually does not improve diagnostic accuracy
for each patient. or alter subsequent evaluation and should therefore be discour-
The acuteness and severity of the presenting symptoms may aged. Finally, administration of small doses of narcotics to patients
help localize the origin of the infection. More important, however, with abdominal pain is unlikely to alter an experienced examiner’s
they allow appropriate triage of these patients, who are frequently diagnostic ability for the worse.
seen in a crowded emergency department. For example, a patient Occasionally, a young patient whose history and physical exam-
with sudden onset of severe abdominal pain and physiologic ination (including vital signs) fit the classic clinical picture of
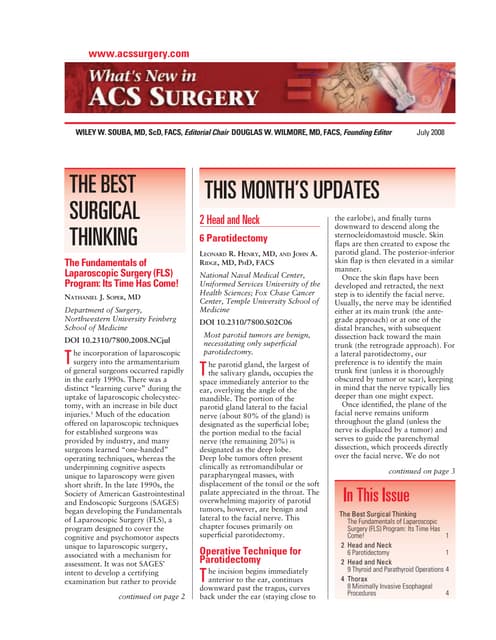
derangement must take precedence over almost all other patients, appendicitis may be taken to the OR without further assessment.](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-1-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 2
Recognition and Management of
Intra-abdominal Infection
Patient has suspected intra-abdominal
infection
Obtain history, including previous surgical
manipulation of abdomen.
Perform physical examination, focusing on
abdomen, pelvis and vagina, and rectum
(inspection, auscultation, percussion, palpation).
Order blood tests as appropriate.
• General tests of systemic response to
infection
• Specific tests to localize source or focus
of infection
On occasion, a young patient with classic
presentation of appendicitis may be taken to
OR without blood tests or imaging.
Order diagnostic imaging as appropriate.
Patient has “certain“ History and physical exam warrant Patient has upper abdominal All other patients
appendicitis exploration of abdomen for peritonitis, pain, elevated bilirubin level
but confirmation (free air) is needed or liver function test results, Order abdominal and pelvic
first; or index of suspicion for or history of biliary tract CT scans.
Resuscitate, give antibiotics,
peritonitis is very low disease Treat specific infection as
and take to OR.
appropriate [see Figure 9].
Order upper abdominal US.
Obtain plain abdominal films, including
upright chest film. Treat specific infection as
appropriate [see Figure 1].
Free peritoneal air is present No free peritoneal air is present, No free peritoneal air is present,
and index of suspicion for but index of suspicion for
Resuscitate, give antibiotics, peritonitis is low peritonitis is high
and take to OR.
Discharge from surgical care. Order abdominal and pelvic CT
scans (see above, right).](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-2-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 3
Practically speaking, however, almost all patients with significant abnormalities, and inflammatory changes. Now that significant
intra-abdominal infections undergo blood tests, and most also intra-abdominal infections—perhaps even in the setting of a per-
undergo some sort of radiologic evaluation. forated viscus—are no longer automatically considered to man-
date operative intervention, the ability of CT scanning to identify
the source and assess the chronicity of an infection is critical to
Investigative Studies effective modern management. Multiple common conditions have
now been defined for which an adequate CT scan allows nonop-
LABORATORY TESTS
erative management either as definitive therapy (e.g., expectant
Blood work can be divided into two treatment of a simple perforated duodenal ulcer) or as a means of
categories: (1) general tests designed to temporizing (e.g., percutaneous drainage of a periappendiceal or
assess the systemic response to infection peridiverticular abscess). In addition, in experienced hands, a neg-
and (2) specific tests designed to localize ative CT scan of the abdomen and the pelvis virtually excludes
the source or site of infection.The former any significant acute surgical illness.
category includes serum chemistries and hematology studies. The It must be noted, however, that a CT scan is not necessary in
latter category commonly includes amylase and lipase concentra- all patients with abdominal pain, and the decision whether to
tions (in patients suspected of having pancreatitis), bilirubin levels obtain one should be made on the basis of predefined guidelines
and liver function tests (to evaluate hepatic or biliary tract disease), or with the input of a general surgeon. When the need for opera-
and lactate levels (when an ischemic bowel is suspected). These tive intervention has already been determined, as in a classic case
tests are discussed further elsewhere, in connection with specific of appendicitis, imaging is unnecessary. In addition, some patients
infections (see below). Urinalysis, of course, is necessary whenever with an intra-abdominal infection amenable to nonoperative man-
urinary tract infection or urolithiasis is a possibility. agement (e.g., simple, mild diverticular disease that can be treat-
ed with oral antibiotics on an outpatient basis) do not necessarily
DIAGNOSTIC IMAGING
benefit from CT scanning.
The use of various radiologic studies In selected cases, other forms of imaging may be used.
in the diagnosis of intra-abdominal infec- Magnetic resonance imaging, though usually more difficult to
tion continues to evolve rapidly. Outside obtain in an emergency and logistically more complicated than
the setting of trauma, it is now very rare CT scanning, yields excellent tomographic images and has the
for patients to undergo operations or added benefit of imaging vascular structures and the pancreatico-
other major interventions without first biliary tree more precisely. Nonetheless, MRI has no significant
undergoing imaging. At one time, plain role in the evaluation of acute peritonitis. Nuclear medicine scans
films of the abdomen (including an and fluoroscopic studies, though occasionally useful adjuncts for
upright chest film) were routinely obtained whenever a significant evaluating biliary tract and upper GI disorders, also play no role
intra-abdominal infection was suspected, principally to detect free in the assessment of acute peritonitis.
peritoneal air, bowel obstruction, or fecaliths. Abdominal plain
films proved to lack sensitivity, specificity, and anatomic definition
in this setting and consequently have, in many cases, been sup- Options for Intervention
planted by abdominal and pelvic computed tomographic scanning. Once an intra-abdominal infection is diagnosed, there are mul-
There are, however, two circumstances in which plain films of the tiple options for intervention. Not infrequently, an approach com-
abdomen remain a reasonable first study for a patient with sus- bining several modalities is warranted. Occasionally, administration
pected peritonitis: (1) when the surgeon has almost decided, on the of systemic antibiotics is all that is necessary (or practical), as in
basis of the history and physical examination, to explore the patient cases of spontaneous primary bacterial peritonitis or of multiple
yet needs confirming evidence of perforation (i.e., free air), and (2) infected fluid collections that are small but too numerous to drain.
when the index of suspicion for peritonitis is so low that the plain Single abscesses, particularly those without thick or particulate
film studies are intended to rule out an unexpected positive finding contents, can be adequately treated with simple aspiration and a
and will not be followed by an abdominal CT scan if negative. short course of antibiotics. For discrete infected fluid collections in
Ultrasonography for intra-abdominal infection is useful only for almost any setting, placement of a percutaneous indwelling drain
focused examination of specific organ systems; it is inferior to CT (most commonly under radiologic guidance) is currently the treat-
scanning for generalized surveillance of the abdomen because of ment of choice. Operative management, either open or laparo-
the inability of sound waves to penetrate gas in the bowel. By far scopic, is employed for resection of damaged or inflamed and
the best-delineated use of ultrasonography is in the diagnosis of unsalvageable organs, diversion of enteric contents, or drainage of
liver and biliary tract disease, for which its ability to demonstrate collections that are too thick or numerous for percutaneous
cholelithiasis makes it superior to CT and for which it should drainage. Beyond these general guidelines, therapy for specific
almost always be the first radiologic test in the appropriate cir- intra-abdominal infections must be individualized (see below).
cumstances (e.g., a classic history of biliary colic or an elevated
serum bilirubin level). Ultrasonography also visualizes the spleen,
the kidneys, and the gynecologic pelvic organs well and has the Infections of the Upper Abdomen
additional benefit of using no ionizing radiation. Biliary tract and pancreatic infections present as a systemic sep-
The abdominal and pelvic CT scan, appropriately, has become tic response or as infections localized in the upper abdomen [see
the key diagnostic test for evaluating patients with suspected peri- Figure 1].Typical findings include abdominal pain, a tender upper
tonitis. This modality is widely available throughout much of the abdominal mass, fever and leukocytosis, and jaundice. Various
world, and newer scanners yield significantly higher resolution combinations of these symptoms may occur, but it is convenient
than older ones, with reduced scanning times and radiation expo- to consider three common clinical presentations. In each of the
sure. CT is highly sensitive for free air, fluid collections, bowel wall presentations, one or two symptoms dominate: (1) upper abdom-](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-3-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 4
Patient has clinical signs of upper abdominal infection,
or serum bilirubin or liver function tests are suggestive
Order abdominal US.
Upper abdominal pain and Fever and jaundice are Fever and abdominal
fever are dominant findings dominant findings mass are dominant
findings
US is normal Stones are seen in Evidence of acute Patient has choledocholithiasis
gallbladder without cholecystitis is apparent or biliary dilation consistent
evidence of with cholangitis
Consider nonbiliary
cholecystitis or If US is equivocal,
disease, especially Resuscitate, and give antibiotics.
choledocholithiasis consider nuclear
acute pancreatitis.
medicine scanning. Consider emergency
Consider abdominal Consider other endoscopic, radiologic, or
Resuscitate; take to OR
and pelvic CT scans. diagnoses. operative biliary drainage.
for urgent cholecystec-
Evaluate for elective tomy if patient is medi-
cholecystectomy. cally fit, or perform
percutaneous drainage
if not.
Patient has liver mass, with Patient has signs of Patient has splenic mass,
or without abscess pancreatic infection with or without abscess
Obtain travel history and Confirm diagnosis via abdominal Confirm diagnosis via abdominal
serologic tests to rule out amebic CT scan. CT scan.
and echinococcal abscesses. Resuscitate, and give antibiotics if Resuscitate, and give antibiotics.
For bacterial abscesses, infection is probable or necrosis Treat with splenectomy or
resuscitate, give antibiotics, is noted on CT. percutaneous drainage.
seek sources, and perform Discrete fluid collection: Aspirate
percutaneous drainage. or drain.
Phlegmon: Attempt medical
management. If unsuccessful and
percutaneous aspirate positive
for bacteria, perform open
Figure 1 Algorithm outlines approach to patient with drainage.
suspected upper abdominal infection.
inal pain and fever, (2) fever and jaundice, and (3) an upper abdominal ultrasound examination: an abnormal image of the
abdominal mass and fever. These clinical findings signal the need gallbladder or bile ducts supports a biliary etiology [see Figure 2].
for a battery of screening tests, including a complete blood count The differential diagnosis should include acute cholecystitis,
(CBC); routine blood tests of liver function; determination of biliary colic, acute pancreatitis, and acute cholangitis, each of
serum amylase level, prothrombin time (PT), and partial throm- which requires specific management [see Table 1]. For example, ini-
boplastin time (PTT); blood culture; chest and abdominal x-rays; tial management of biliary colic and mild acute pancreatitis is usu-
and abdominal ultrasonography. When considered together, the ally nonoperative, whereas severe acute cholangitis and acute
clinical findings and the test results allow early differentiation of cholecystitis are treated by means of surgical, endoscopic, or radi-
the three most common disease entities: acute cholecystitis, acute ologic intervention (see below). Clinical features and blood test
cholangitis, and acute pancreatitis. results, though helpful, may be inconclusive.The abdominal ultra-
sonogram may provide specific clues. Stones appear in biliary colic
UPPER ABDOMINAL PAIN AND FEVER
[see Figure 2]; stones and thickening of the gallbladder wall, in
Patients with upper abdominal sepsis may present with epigas- acute cholecystitis; gallstones and dilatation of the common bile
tric or right upper quadrant pain and fever. Only two thirds of duct (CBD), in acute cholangitis; and pancreatic enlargement and
these patients admitted with a working diagnosis of acute chole- sonolucency, in pancreatitis.
cystitis have acute biliary inflammation.1 In some patients, non-
surgical conditions (e.g., pneumonia, acute hepatitis, familial Pancreatitis
Mediterranean fever, herpes zoster of the intercostal nerves, and Diagnosis Differentiating acute pancreatitis from acute
gastroenteritis) can be distinguished clinically from biliary disease. cholecystitis may be difficult.The serum amylase level lacks speci-
The most important screening test for acute biliary infection is the ficity, but if the clinical findings suggest acute pancreatitis, an ele-](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-4-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 5
Table 2—Ranson’s Early Objective Signs
of Severity of Acute Pancreatitis2
On Admission After Initial 48 Hours
Age > 55 yr Serum Ca2+ < 8 mg/dl
Glucose > 200 mg/dl Arterial PO2 < 60 mm Hg
WBC > 16,000/mm3 Base deficit > 4 mEq/L
LDH > 350 IU/L BUN increase > 5 mg/dl
Hematocrit fall > 10%
AST > 250 Sigma Frankel U/dl
Fluid sequestration > 6,000 ml
Note: < 3 signs = mild pancreatitis; ≥ 3 signs = severe pancreatitis.
AST—aspartate aminotransferase—BUN—blood urea nitrogen—PO2—oxygen tension—
WBC—white blood cell
acute pancreatitis.5,6 Unless clinical findings and the results of bio-
chemical tests and ultrasonography are unequivocal, a contrast-
enhanced spiral abdominal CT scan is usually performed to estab-
lish the diagnosis and stage acute pancreatitis. It has been sug-
gested, however, that CT scanning should be reserved for patients
with clinically suspected severe acute gallstone pancreatitis, on the
grounds that the results would not change the recommended
course of action in other patients.7 Occasionally, a very mild pan-
creatitis may give rise to no findings on a CT scan, and a normal
technetium-99m (99mTc)–labeled HIDA (lidofenin) scan may help
differentiate this condition from acute cholecystitis.
Figure 2 Abnormal abdominal ultrasound examination shows Treatment Given that pancreatitis encompasses a wide
calculi in gallbladder casting shadows on underlying liver tissue. range of diseases with varying degrees of severity, treatment must
be individualized for each patient. Possible therapeutic strategies
range from outpatient management with temporary dietary mod-
vated level of serum amylase clinches the diagnosis. In one study, ification (for very mild cases) to open debridement and complex
the initial laboratory results in 100 patients with acute pancreati- intensive care (for severe cases). It is therefore useful to base pos-
tis were compared with those in 100 patients with acute abdomi- sible treatment approaches in particular cases on the cause and
nal pain caused by acute cholecystitis, perforated peptic ulcer, or severity of the pancreatitis.
acute appendicitis.2 The serum amylase concentrations were ele- Gallstone pancreatitis. Standard therapy for gallstone pancreatitis
vated in 95% of patients with acute pancreatitis but were normal includes I.V. fluids and narcotic analgesics. Nasogastric suction is
in 95% of patients with acute abdominal pain from other causes. useful in patients with significant ileus but need not be used rou-
These concentrations peak within the first 48 hours and are tinely.8 The use of systemic antibiotics is controversial; they are of
almost always elevated in biliary pancreatitis3; in fact, a serum benefit in the 10% to 34% of patients who have concomitant
amylase concentration above 1,000 U/L strongly suggests a biliary cholangitis.9 Other treatments suggested previously—including
origin of the pancreatitis.4 In addition, determination of serum total parenteral nutrition (TPN) and various pharmacologic agents
lipase levels has been shown to be more specific than and at least (e.g., cimetidine, somatostatin, glucagon, and insulin)—have not
as sensitive as determination of amylase levels for the detection of proved useful in all cases of gallstone pancreatitis.10 Continuous
intraduodenal infusion of an elemental diet has reduced exocrine
pancreatic secretions in animal experiments.11 Furthermore, enter-
Table 1—Diagnostic Indicators of al feeding has been shown to be beneficial and to decrease disease
Upper Abdominal Pain and Fever severity in patients with acute pancreatitis.12-14
In clinical practice, the need for further treatment depends on
Acute Acute the severity of the acute pancreatitis. Severity determines both the
Biliary Colic
Cholecystitis Pancreatitis risk of sepsis, which governs outcome, and the risk associated
with early cholecystectomy [see 5:21 Cholecystectomy and Bile Duct].
Short: 40%
Duration
< 1 hr
Persistent Persistent The most commonly used clinical prognostic index in North
America was developed by Ranson and reliably defines the sever-
Pathogenesis Visceral Somatic Retroperitoneal
ity of pancreatitis [see Table 2].2 In mild pancreatitis, one or two
Guarding and Guarding and Ranson signs are present; in more severe pancreatitis, three to five
Signs Tender
spasm spasm signs are present; and in very severe pancreatitis, more than five
Laboratory tests signs are present. This distinction serves to stratify further treat-
Liver function tests Occasionally Abnormal Abnormal ment. Other clinical prognostic scores, such as the APACHE-II
abnormal (Acute Physiology and Chronic Health Evaluation II) and
Serum amylase Normal Normal or slightly Increased APACHE-III scores and the Balthazar score, have been shown to
increased
Leukocyte counts Often normal Increased Increased
possess discriminatory value in identifying patients at high risk for
complications.15,16](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-5-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 6
Mild pancreatitis usually subsides within 1 week of onset. Most cholecystectomy has facilitated this approach safely without pro-
surgeons defer cholecystectomy until then; urgent operation should longing hospital stay.
be reserved for cases complicated by biliary sepsis, and it may Severe pancreatitis. Patients with three or more Ranson signs are
reveal acute cholecystitis in as many as 31% of patients.17 at particular risk for pancreatic sepsis.28 Repeated clinical and
An attack of acute gallstone pancreatitis is initiated by obstruc- radiologic evaluation is required in these patients to ensure early
tion at the confluence of the lower end of the CBD and the pan- detection of complications, because the outcome of an episode of
creatic duct by a stone or by edema at the ampulla of Vater result- pancreatitis depends on whether sepsis supervenes. When infec-
ing from stone migration. These stones may be found and tion occurs, operative debridement and drainage are required [see
removed in 63% to 78% of patients who undergo operation with- Fever and Abdominal Mass, below]. Some surgeons have attempt-
in 72 hours of admission17-19 [see 5:22 Biliary Tract Disease]; by ed to alter the course of severe disease by early operation; howev-
contrast, they are present in only 3% to 33% of patients explored er, urgent operation is associated with a high mortality in patients
after the first week.18-22 A randomized trial exploring the optimal with more than three Ranson signs.19,21,23,29 To avoid the mortali-
timing of surgery for gallstone pancreatitis showed that early ty associated with early operative intervention, some clinicians
surgery (within 48 hours after admission) was not associated with advocate early diagnosis by ERCP [see Figure 3], followed by bil-
a significant increase in morbidity or mortality in patients with iary decompression by means of endoscopic sphincterotomy and
mild pancreatitis but did not change prognosis.23 stone extraction. In a randomized trial comparing early ERCP and
Endoscopic retrograde cholangiopancreatography (ERCP). Early sphincterotomy with conservative therapy in patients with severe
ERCP and sphincterotomy [see 5:18 Gastrointestinal Endoscopy] has acute pancreatitis, ERCP and sphincterotomy decreased morbid-
been suggested as an alternative to surgery of the CBD in patients ity from 61% to 24% and lowered mortality from 18% to 4%.24
with mild pancreatitis. However, randomized trials comparing The results of this trial, however, have been the subject of debate,
endoscopic treatment with conservative treatment within the first and the success of this approach has been attributed by some
72 hours in patients with mild pancreatitis did not find that urgent authors to the treatment of a concomitant cholangitis rather than
endoscopic sphincterotomy improved outcome in this group of of the actual pancreatitis.25 A well-conducted trial that excluded
patients.24,25 Other studies showed that delaying surgery beyond 6 patients with concomitant cholangitis was published in 1997;
weeks may lead to a 32% to 57% risk of recurrent pancreatitis.26,27 unfortunately, this trial was unable to answer the question defini-
Therefore, cholecystectomy and cholangiography should be tively, because too few patients with severe pancreatitis had been
delayed only until just before patients are discharged from the hos- recruited.30 It appears that ERCP is warranted mainly in cases of
pital, 5 to 15 days after the onset of symptoms. Laparoscopic acute pancreatitis complicated by cholangitis and biliary sepsis.31,32
Use of peritoneal lavage in early severe pancreatitis was advo-
cated in one study to decrease morbidity and mortality.33 Use of
standard lavage over a 2-day period did not improve patient out-
come, but use of peritoneal lavage for 7 days (long peritoneal
lavage) yielded some improvement in outcome.34 Early use of
antibiotics and selective decontamination have been proposed as a
means of reducing septic complications, but neither has convinc-
ingly or reproducibly been shown to improve prognosis.35,36
Although prophylactic antibiotics have been shown to decrease the
rate of infectious complications in severe acute pancreatitis, they
have not clearly been shown to reduce overall disease mortali-
ty.35,37-40 Attempts have been made to modulate the initial systemic
inflammatory response seen in early severe acute pancreatitis to
reduce the risk of subsequent infection and improve overall prog-
nosis; somatostatin has exhibited limited success in this regard.41,42
Another drug in this category, the platelet-aggregating factor
(PAF) inhibitor lexipafant, initially yielded promising results in
animal models43,44 and in phase II trials45; however, a 2001 trial
using the same drug did not find it efficacious for treating severe
acute pancreatitis.46
Acute Cholecystitis
Diagnosis Acute cholecystitis is the most common diagnosis
in patients presenting with upper abdominal pain and fever and is
characterized by the clinical finding of a midinspiratory arrest on
palpation of the right upper quadrant (Murphy’s sign). As noted
(see above), with the widespread availability of ultrasonography,
acute cholecystitis can usually be diagnosed rapidly on the basis of
the findings of gallbladder wall thickening, pericholecystic fluid,
and stones. Occasionally, more complex cases must be evaluated
Figure 3 Endoscopic retrograde cholangiopancreatography with nuclear medicine scanning to look for cystic duct obstruc-
shows distal CBD stone in acute pancreatitis. Papillotome has tion. Concurrent acute obstructive cholangitis must also be con-
been placed through sphincter of Oddi in preparation for endo- sidered in all patients with acute cholecystitis. Supportive labora-
scopic sphincterotomy. tory data include a high serum bilirubin level and an increased](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-6-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 7
Table 3—Comparison of Acute Cholecystitis
and Emphysematous Cholecystitis
Emphysematous
Acute Cholecystitis
Cholecystitis
Gender 70% male 70% female
Stones 70% 90%
Bile culture positive 95% 66%
Clostridia found 46% 1.2%
Gangrenous gallbladder 75% 2.5%
Perforation of gallbladder 20% 4%
Mortality at age < 60 yr 15% 1.5%
Pathogenesis Ischemia, obstruction Obstruction
sustained narcotics therapy). In addition, focal inflammation may
cause biliary colonization or may activate coagulation factor XII,
thereby causing severe injury to the blood vessels in the gallblad-
der muscularis and serosa. A high index of suspicion is necessary.
Acute acalculous cholecystitis should be considered in any post-
operative or acutely ill patient with upper abdominal pain and
Figure 4 Air outlines gallbladder and bile ducts in emphysema-
fever or with unexplained fever and leukocytosis. It is particularly
tous cholecystitis.
common 2 to 4 weeks after injury. The diagnosis is confirmed by
findings on abdominal ultrasound examination [see Figure 5] and
99m
alkaline phosphatase level. Positive blood cultures and dilated Tc-labeled HIDA scanning coupled with infusion of cholecys-
biliary ducts on abdominal ultrasonography usually confirm the tokinin and morphine.52-54
diagnosis.
Emphysematous cholecystitis. An uncommon and insidious vari- Treatment Standard treatment of acute cholecystitis consists
ant of acute cholecystitis, emphysematous cholecystitis is charac- of I.V. fluid administration, analgesics, and cholecystectomy.
terized by gas in the gallbladder lumen or wall or in the perichole- Although the timing of operation is somewhat controversial in
cystic soft tissue and biliary ducts secondary to gas-forming bac- ordinary acute cholecystitis, cholecystectomy should be per-
teria.The key to the diagnosis is the presence of air on abdominal formed at the earliest opportunity [see 5:21 Cholecystecomy/Bile
x-ray [see Figure 4] or ultrasound examination. Three stages of Duct]. This approach has been confirmed by at least one ran-
emphysematous cholecystitis have been defined: (1) gas is seen domized trial comparing early with late laparoscopic cholecystec-
only in the lumen of the gallbladder, (2) a ring of gas is identified tomy.55 The delayed-surgery group had a greater need for conver-
in the wall of the gallbladder, and (3) gas is seen in the tissues adja- sion to open cholecystectomy (23% versus 11%), as well as a longer
cent to the wall. Compared with ordinary acute cholecystitis,
emphysematous cholecystitis is associated with a fivefold increase
in the risk of gallbladder perforation, as well as a 10-fold increase
in mortality in patients younger than 60 years [see Table 3].47
Studies from the 1960s noted an increased risk of gangrene and
perforation of the acutely inflamed gallbladder in patients with
diabetes mellitus.48,49 The mortality for acute cholecystitis was also
shown to be five to 10 times higher in patients with diabetes than
in other patients. Later studies, however, did not show an in-
creased mortality in patients with both diabetes and acute chole-
cystitis.50,51 Nevertheless, one third of patients with emphysema-
tous cholecystitis also have diabetes.This factor, coupled with the
current tendency to perform cholecystectomy early in most pa-
tients with acute cholecystitis, may account for the disparity be-
tween previous studies and later reports.
Acute acalculous cholecystitis. Another variant of acute cholecys-
titis is acalculous cholecystitis; though still rare, it became more
common from the 1950s through the 1990s.This disease was orig-
inally described as occurring after surgical treatment of unrelated
disease but was subsequently identified in patients with multiple Figure 5 Abnormal abdominal ultrasound examination con-
trauma, prolonged critical illness, and sepsis. Predisposing factors firms diagnosis of acute acalculous cholecystitis. When image is
include gallbladder ischemia (in patients with shock or trauma) compared with that in Figure 2, thickening of gallbladder wall
and biliary stasis (in prolonged fasting, hyperalimentation, and and intraluminal debris are obvious.](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-7-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 8
average total hospital stay and convalescence. Administration of jaundice, with pain a less marked component. Jaundice is almost
systemic antibiotics is not required; however, single-dose antibiot- always associated with obstruction of the biliary tree, either intra-
ic prophylaxis (e.g., cefazolin, 2 g I.V.) can be given at the start of hepatic or extrahepatic. The combination of fever with jaundice
the operation [see 1:1 Prevention of Postoperative Infection].56-58 always suggests acute cholangitis, a condition that can have a ful-
Some patients with acute cholecystitis are at high risk for gan- minant and fatal course if not treated promptly.
grene and perforation of the gallbladder. It is crucial to identify
these patients and perform cholecystectomy promptly because Acute Cholangitis
delay increases morbidity and mortality. Clinically, gangrene and Diagnosis If a patient presents with a temperature higher
perforation of the gallbladder in this high-risk population are sug- than 38.5º C (101.3º F) in conjunction with jaundice [see 5:3
gested by marked systemic toxicity or by the radiologic demon- Jaundice], the possibility of acute cholangitis should always be
stration of either emphysematous cholecystitis or acute acalculous investigated. If cholangitis is present, laboratory studies will reveal
cholecystitis. leukocytosis, and blood cultures will often be positive. A finding of
With ordinary acute cholecystitis, body temperature is slightly gallstones and dilated biliary ducts on abdominal ultrasound exam-
increased in most patients—averaging 37.8º C (100.04º F)—but ination supports the diagnosis. Reynolds’ pentad is present in the
is normal in 20% of patients. By comparison, the risk of gangrene full-blown syndrome.66 This syndrome includes upper abdominal
and perforation is reportedly higher in patients with marked sys- pain, fever and chills, jaundice, hypotension, and mental status
temic toxicity, manifested by a pulse rate greater than 120 changes. Acute cholangitis is usually related to choledocholithiasis,
beats/min, a body temperature higher than 39º C (102.2º F), and recent biliary manipulation, or biliary stenting performed for chron-
a left shift in the differential white blood cell count, showing more ic obstruction.
than 90% polymorphonuclear leukocytes. Unfortunately, findings Gallbladder infections. Gallbladder empyema can duplicate most
of systemic toxicity are frequently absent in elderly patients. of the findings associated with acute cholangitis. In this condition,
Patients with acute cholecystitis who have signs of systemic tox- acute cholecystitis is complicated by suppuration within the gall-
icity, emphysematous cholecystitis, or acalculous cholecystitis are bladder, which then becomes the focus of generalized sepsis. The
at high risk for gallbladder gangrene and perforation and therefore distended gallbladder may be palpable and tender.When jaundice
require prompt and aggressive treatment. I.V. antibiotic therapy is associated with empyema of the gallbladder, it is less likely to be
with a single agent (e.g., ceftriaxone, piperacillin, or a quinolone obstructive than when it is associated with acute cholangitis.True
such as ciprofloxacin or ofloxacin) can be given.59,60 Early chole- empyema of the gallbladder is rare. Treatment includes adminis-
cystectomy is the treatment of choice. Unfortunately, mortality tration of I.V. fluids, systemic antibiotic therapy, analgesics, and
may be as high as 20% to 30% with the traditional surgical ap- early cholecystectomy.
proach.61 If perforation and gangrene are not suspected but med- In some patients with jaundice and inflammation, a stone
ical illness poses a high risk of mortality from operation, nonoper- impacted in the cystic duct or in Hartmann’s pouch may suggest
ative supportive therapy may suffice. If this fails, another treatment choledocholithiasis, but preoperative diagnosis by ERCP shows an
option is cholecystostomy. extrinsic compression of the duct known as Mirizzi syndrome.Two
Percutaneous transhepatic cholecystostomy has been recom- types of Mirizzi syndrome exist. In type I, a stone impacted in the
mended for these high-risk patients,62 particularly where there is a cystic duct or Hartmann’s pouch compresses the common hepatic
low risk for perforation of the gallbladder.63 To determine the risk duct and causes inflammation, thereby leading to jaundice.
of gallbladder perforation, a risk score can be assigned to each of Treatment of this type consists of obliteration of the cystic duct and
seven findings that may be present on the preoperative abdominal careful partial cholecystectomy, with the neck of the gallbladder left
ultrasound examination: pericholecystic fluid, 7 points; distention in place. In type II, protrusion of the stone into the hepatic duct
of the gallbladder, 4 points; intraluminal membrane, 4 points; erodes the septum between the cystic duct and the hepatic duct
intraluminal debris, 3 points; round gallbladder, 3 points; sonolu- and causes a cholecystocholedochal fistula. Treatment of this type
cent zone in the gallbladder wall, 2 points; and a thick gallbladder involves internal biliary drainage to the wall of the cholecysto-
wall (> 3.5 mm), 1 point.63 A patient with a total risk score of 12 choledochal defect, usually with a choledochojejunostomy [see 5:22
or more points requires urgent cholecystectomy; one with a lower Biliary Tract Disease], in addition to cholecystectomy.67
score who does not respond to conservative treatment may be Primary sclerosing cholangitis. Patients with primary sclerosing
treated with percutaneous transhepatic cholecystostomy. cholangitis, especially those who have undergone internal or exter-
A 1997 review of 59 patients exhibiting the septic response who nal biliary drainage, are at high risk for recurrent bouts of ascend-
underwent successful percutaneous radiologic cholecystostomy ing cholangitis. Primary sclerosing cholangitis predominantly affects
defined predictors of a successful clinical outcome: localized right young males, particularly those with chronic ulcerative colitis.The
upper quadrant tenderness and gallstones, as well as gallstones diagnosis is suggested by the dominant cholestatic biochemical
and pericholecystic fluid on ultrasound examination.64 Patients profile—that is, elevation of the serum bilirubin concentration, the
with more equivocal findings may derive greater benefit from serum alkaline phosphatase level, and aspartate aminotransferase
more invasive techniques that can simultaneously be used for activity. Because of the concomitant hepatic scarring, ultrasonog-
diagnostic purposes (e.g., laparoscopy, which can even be per- raphy may not reveal the presence of dilated intrahepatic ducts.
formed at the ICU bedside65). Definitive diagnosis requires visualization of the beaded appear-
A few patients with acute cholecystitis will have concurrent ance of the biliary tree by means of cholangiography. Cholangio-
acute cholangitis. Cholecystostomy is contraindicated in these carcinoma and secondary sclerosing cholangitis in patients with
patients because of its high mortality; adequate drainage of the Caroli disease or choledochal cysts may mimic these clinical, bio-
CBD is required in such cases [see Fever and Jaundice, below]. chemical, and radiologic features, but this is an unusual occur-
rence and can be distinguished by careful follow-up of patients.
FEVER AND JAUNDICE
Currently, magnetic resonance cholangiopancreatography
An alternative presentation of upper abdominal infection (MRCP) is the imaging modality of choice for elective manage-
includes patients whose predominant symptoms are fever and ment of patients with primary sclerosing cholangitis, in that it yields](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-8-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 9
results comparable to those of ERCP without being invasive.68-71 decompression in these critically ill patients can result in a mor-
Other causes of cholangitis. An uncommon cause of recurrent tality of 30% to 40%.82-85 Furthermore, reoperation is required in
cholangitis in North America is Oriental cholangiohepatitis, which one third of survivors because important diagnostic information is
is characterized by intrahepatic duct scarring, biliary strictures, not available at the initial laparotomy. As a result, nonoperative
and hepatolithiasis, as demonstrated by cholangiography. Irrever- methods of biliary decompression, including percutaneous trans-
sible intrahepatic and extrahepatic liver damage may result be- hepatic biliary drainage (PTBD) and endoscopic sphincterotomy
cause of the overwhelming propensity of these patients to form at ERCP, have gained favor. PTBD was originally developed for
calcium bilirubinate stones. preoperative management of biliary obstruction without cholangi-
A few patients with cholangiocarcinoma causing bile duct ob- tis but has not been found to be beneficial in that setting. At pres-
struction or liver metastases causing intrahepatic bile duct obstruc- ent, it is mainly used for the management of proximal bile duct
tion may also present with a clinical picture suggestive of cholan- strictures or for the treatment of cases not amenable to ERCP; its
gitis. CT followed by MRCP can delineate the diagnosis in most complication rate is less than 10%.86
such cases.Treatment consists of I.V. antibiotics and biliary drain- Although PTBD can reduce the mortality associated with ini-
age by radiographic or surgical means. tial biliary decompression, many patients still require a definitive
operation. Consequently, endoscopic sphincterotomy [see 5:18 Gas-
Treatment Once acute cholangitis is diagnosed, resuscita- trointestinal Endoscopy] has been proposed for decompression of
tion is started with I.V. fluids and antibiotics, such as fluoro- the biliary tree in patients with acute cholangitis from choledo-
quinolones, mezlocillin, cefoperazone, or piperacillin,59,72-75 partic- cholithiasis [see Figure 6]. In a study of 82 patients with acute
ularly in patients with marked hyperbilirubinemia, in whom treat- cholangitis caused by CBD calculi, early operation was employed
ment with aminoglycosides may contribute to renal toxicity in up in 28 patients, endoscopic sphincterotomy in 43, and antibiotic
to 33% of cases [see 8:6 Renal Failure].76 These antibiotics are therapy alone in 11.87 Surgical mortality was 21% and morbidity
required to deal with the various aerobic bacteria, of which 57%; by comparison, mortality for endoscopic sphincterotomy
Escherichia coli, Klebsiella species, and enterococci are the most fre- was 5% and morbidity 28%. Others confirmed these findings.81 In
quently encountered in this setting. Anaerobes may be isolated in patients whose gallbladder is still in place, endoscopic sphincter-
15% to 30% of patients and are particularly likely to be present in otomy alone, without cholecystectomy, may even be a reasonable
diabetics, the elderly, and patients who have previously undergone long-term option. Of 23 patients whose gallbladders were left in
biliary manipulation. In patients with indwelling catheters, situ,87 only two required cholecystectomy in the 1- to 7-year fol-
Enterobacter, Pseudomonas, and Candida organisms are being isolat- low-up period: one for empyema of the gallbladder and one for
ed with increasing frequency. Indications of high risk include a recurrent cholangitis.
serum bilirubin concentration higher than 3 mg/dl. An increasingly recognized cause of cholangitis is biliary sepsis
Approximately 75% of patients with acute cholangitis respond after manipulation of the biliary tree with ERCP or PTBD.
to conservative measures,77 and supportive treatment is contin- Treatment includes I.V. fluids and antibiotics. To prevent this
ued. Subsequent investigations usually include CT followed by complication, prophylactic antibiotics should be administered be-
MRCP.78,79 Because of their invasive nature, ERCP and needle fore every biliary manipulation.88
percutaneous transhepatic cholangiography (PTC) are reserved
FEVER AND ABDOMINAL MASS
for cases in which a drainage procedure is anticipated or the infor-
mation from the MRCP is deemed inadequate. A third group of patients with upper abdominal infection pre-
For the 25% of patients who do not respond to conservative sent with fever and an upper abdominal mass identified either by
treatment, early recognition may improve their prognosis. In one clinical signs or through diagnostic imaging. Even if the mass is
study, patients who did not respond immediately to antibiotics only vaguely palpable, the mass effect is demonstrable on ultra-
had a mortality of 62%, compared with a mortality of 1.5% in sound examination of the abdomen. If the abdominal ultrasound
those who improved.80 In another study, indicators of high risk examination is technically unsatisfactory because of intestinal gas,
were an arterial blood pH less than 7.4, a serum bilirubin con- contrast-enhanced CT of the abdomen will facilitate the diagnosis.
centration above 9 mmol/L, a blood platelet count below The differential diagnosis is aided by the location of the mass.
150,000/mm3, and a serum albumin concentration lower than 3 A mass in the right upper quadrant usually indicates acute chole-
g/dl.102 These high-risk patients often have systemic hypotension, cystitis, though the possibility of a liver abscess must also be con-
mental confusion, a temperature higher than 39º C (102.2º F), or sidered. A mass in the epigastrium or in the left upper quadrant
hypothermia. Occasionally, acute cholangitis is complicated by dis- usually signals a pancreatic infection; in rare instances, a solitary
seminated intravascular coagulation (DIC), which manifests itself splenic abscess is found. Patients with an intra-abdominal abscess
as a tendency to bruise and bleed or merely as prolongation of the in the subphrenic space or an interloop abscess may also present
PT and the PTT, together with a fall in the blood platelet count in this manner.
[see 1:4 Bleeding and Transfusion]. If DIC is suspected, the diagno-
sis should be confirmed and treatment started before biliary Liver Abscess
decompression. Diagnosis In the setting of acute upper abdominal sepsis, a
Patients with refractory cholangitis who do not improve within tender mass in the right upper quadrant is most likely an enlarged,
24 hours require urgent biliary decompression. Urgent biliary inflamed gallbladder, possibly wrapped with omentum [see Upper
decompression had traditionally been accomplished via surgical Abdominal Pain and Fever, Acute Cholecystitis, above]. The next
exploration of the CBD and T-tube drainage [see 5:22 Biliary Tract most common cause of fever and abdominal mass in the right
Disease]. Cholecystostomy is an inadequate and often fatal upper quadrant, however, is liver abscess.
option in this context. Rarely, T-tube insertion alone may be life- Pyogenic abscess. Today, pyogenic liver abscess is most common-
saving in a desperately ill patient; generally, however, definitive ly related to biliary tract obstruction from gallstones or malignant
internal decompression is preferable. Unfortunately, any surgical disorders (35% of cases), and the ultrasound examination may](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-9-2048.jpg)

![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 11
Blood cultures are positive in as many as 50% of patients with a decrease in the size of the abscess is apparent within 1 week on
pyogenic abscess, particularly in those with multiple abscesses; in ultrasonographic examination, though a small residual cavity may
fact, the presence of Streptococcus milleri in the blood suggests a vis- persist for as long as 2 years. If the patient’s condition does not
ceral abscess. improve, needle aspiration and culture are indicated. Secondary
infection is treated as a pyogenic abscess. Otherwise, oral emetine,
Treatment Pyogenic abscess. The preferred treatment of pyo- 65 mg/day, is added for up to 10 days.
genic abscess is closed continuous percutaneous drainage guided Echinococcal abscess. Symptomatic or secondarily infected echi-
by CT or ultrasonography, provided that it is technically feasible nococcal cysts are best treated by means of surgical excision or
and no other indication for laparotomy exists.94 More than one marsupialization. The use of oral anthelmintics (e.g., albendazole
catheter may be required for complete drainage. An alternative and mebendazole) has met with limited success. Nevertheless, pre-
treatment is repeated percutaneous needle aspiration, the results operative treatment with albendazole or mebendazole for 1 month,
of which are comparable to those of continuous drainage.95 One combined with postoperative treatment, is indicated to reduce the
advantage to repeated needle aspiration is the elimination of cum- risk of intraoperative seeding or postoperative recurrence.109,110
bersome, painful drainage tubes, which are prone to dislodgment.
Although initial studies showed a good response rate with repeat- Pancreatic Infection
ed needle aspiration,96 the results were not duplicated in a subse- Diagnosis When the mass is located in the epigastrium or the
quent randomized trial.97 left upper quadrant, a pancreatic source is most likely. Prompt and
The abscess cavity dimensions are followed by serial imaging accurate diagnosis is crucial because severe pancreatic infection is
until the cavity collapses, and the catheter can usually be removed fatal if left untreated.The key to successful treatment is early diag-
2 to 3 weeks later. Continuous percutaneous drainage has been nosis of infected pancreatic necrosis, infected pseudocyst, and pan-
associated with a complication rate of 4% and a failure rate of creatic abscess. A high index of suspicion is required to diagnose
15%.98 However, operative drainage is the treatment of choice in these three infectious processes and to differentiate them from a
patients with an identified intra-abdominal focus of infection and pancreatic inflammatory mass or phlegmon,28 in which pancreatic
in patients in whom percutaneous drainage is not feasible or has edema and inflammation are present without necrosis or infection.
failed.99 Operative drainage, especially via a laparoscopic approach, Correct diagnosis and treatment of infected pancreatic necrosis,
is a highly effective treatment option that is associated with low infected pseudocyst, and pancreatic abscess require an under-
mortality and morbidity.100 In some patients, a limited hepatic standing of their pathophysiology. It is generally assumed that
resection [see 5:23 Hepatic Resection] may be required to eliminate infected pancreatic necrosis develops as a transmural, transductal,
multiple abscesses, particularly when an underlying intrahepatic lymphatic, or hematogenous infection of a necrotic region of the
stricture is the source.101 pancreas. Infection develops in 40% of cases of pancreatic necro-
Treatment of pyogenic liver abscess should include systemic sis, usually in week 2 or 3 after development of the acute pancre-
antibiotic therapy. Approximately 70% of pyogenic liver abscesses atitis.111 Surgical debridement is required in these cases to prevent
yield polymicrobial isolates,102 and 25% to 45% of the organisms death. Pancreatic abscesses form by liquefaction of infected necro-
are anaerobic.103 Multiple anaerobic isolates suggest the colon as a sis.They usually occur after week 5 of pancreatitis, when the acute
source, whereas a single isolate of E. coli suggests a nidus in the bil- phase of the disease has subsided.112 Pancreatic abscesses are asso-
iary tree. Antibiotic treatment should include initial coverage of ciated with a lower mortality than infected pancreatic necrosis.
both aerobes and anaerobes with either a single agent or multiple Like pancreatic abscesses, infected pancreatic collections and
agents.The need to cover enterococci has been debated, but these pseudocysts present late in the course of pancreatitis. They are
organisms clearly are increasingly important nosocomial patho- associated with a lower mortality than pancreatic abscesses.
gens. An acceptable initial treatment regimen consists of a single Caused by infection in 13% of localized collections resulting from
broad-spectrum agent (e.g., ticarcillin-clavulanate or meropenem). ductal blowout, infected pancreatic collections and pseudocysts
It should be noted that significant changes have occurred in the eti- may occur in the pancreas itself, in contiguous peripancreatic tis-
ology, bacteriology, and treatment of liver abscesses. There is a sue, or in remote (extrapancreatic) tissue.
trend toward a higher incidence of pseudomonal and streptococcal Clinical evaluation alone is generally insufficient to diagnose
infections, and the frequency of fungal infection is increasing as pancreatic infection. A clearly defined upper abdominal mass is
well.104 The mortality from this disease remains high, and appropri- palpable in only 50% to 75% of cases.28 In most patients, the
ate antibiotic coverage with drainage is of paramount importance. screening battery of tests reveals leukocytosis with leukocyte
The duration of antibiotic therapy is controversial105; according counts greater than 15,000/mm3. Blood cultures are positive in
to one set of guidelines, antibiotics should be continued for 3 to 4 50% of cases. CT-guided percutaneous aspiration with Gram stain
weeks when the abscess has been excised, 4 to 8 weeks when a soli- and culture provides the best method of diagnosing pancreatic
tary abscess has been drained, and 6 to 8 weeks when multiple infection. In one study of 75 patients with clinical toxicity sugges-
macroscopic abscesses have been drained.106 Multiple microscopic tive of pancreatic sepsis, infection was confirmed in only 40%.113
abscesses usually require that a biliary source also be treated.85 The In another study of 21 patients with pancreatic infection, only five
overall prognosis for multiple small hepatic abscesses is not as good had specific signs on abdominal CT scan.114 CT-guided diagnos-
as that for solitary abscesses, and the development of a pyogenic tic needle aspiration leads to a correct diagnosis within 72 hours
abscess in a patient with an underlying hepatobiliary or pancreatic in two thirds of patients, and the mortality associated with opera-
malignancy has been identified as a preterminal event associated with tive intervention is 19%; however, CT-guided needle aspiration is
a hospital mortality of 28% and survival of less than 6 months.107 beneficial only if pancreatic infection is suspected and if the tech-
Amebic abscess. Medical treatment is now the standard approach nique is used early in the course of disease.
to management of amebic liver abscesses. Metronidazole, 750 mg Several laboratory markers of pancreatic necrosis have been
orally three times a day for 10 days, is a highly effective regimen.108 investigated, such as serum methemalbumin, serum ribonuclease,
A favorable response to treatment occurs within 4 to 5 days, and and C-reactive protein. Most of these markers are too insensitive](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-11-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 12
for routine clinical practice. However, serum levels of C-reactive pseudocysts can usually be treated nonoperatively. In one prospec-
protein above 10 mg/dl have been reported to be 95% accurate in tive study, percutaneous and surgical drainage were equally suc-
predicting necrosis.115 cessful in treating infected pancreatic fluid collections and pseudo-
Currently, the best indicators of infected pancreatic necrosis or cysts.124 Clinical signs of progress rather than CT findings are the
abscess are a combination of Ranson’s objective prognostic signs best indicators of the need for intervention, and nonoperative
[see Table 2] and dynamic abdominal CT scan findings. In Ranson’s methods should be attempted before open surgery is planned.
series, the pancreatic findings on CT were graded in five categories Adjunctive procedures. In the past, debridement and sump
[see Figure 7]116: (a) normal, (b) pancreatic enlargement alone, (c) drainage were accompanied by the so-called triple ostomy tech-
inflammation of the pancreas and peripancreatic fat, (d) one peri- nique, which involved cholecystostomy, gastrostomy, and jejunos-
pancreatic fluid collection, and (e) two or more peripancreatic fluid tomy. The role of these ancillary procedures, however, is contro-
collections. Only category e was associated with a high (61%) inci- versial at best, and currently, cholecystostomy is employed only if
dence of pancreatic abscess. The number of objective prognostic gallstones are detected.
signs present also predicted the subsequent development of an Other operative procedures may be required to manage gastric
abscess: fewer than three signs, 12.5%; three to five signs, 31.8%; or colonic complications. Gastric bleeding, gastric outlet obstruc-
and more than five signs, 80%. However, the value of this method tion, and gastric fistula necessitating reoperation are relatively
was limited because only five of the 83 patients evaluated had more infrequent in this setting. By contrast, colonic necrosis and fistula
than five prognostic signs. By combining the objective prognostic formation are relatively common and occur either spontaneously
signs with positive abdominal CT findings, the investigators identi- or as complications of treatment. The usual site of involvement is
fied 30 patients who had three or more objective signs and were the splenic flexure or upper descending colon.Treatment consists
graded as category c, d, or e on abdominal CT scan; in these of colonic resection or a diverting colostomy [see 5:34 Laparo-
patients, the incidence of pancreatic abscess was 56.7%. By con- scopic Coloctomy].
trast, no patient with fewer than three prognostic signs and graded Antibiotic therapy.The role of systemic antibiotic therapy in the
as category a or b on abdominal CT scan had a pancreatic abscess. prophylaxis of pancreatic abscess is controversial. Experimental
evidence suggests that antibiotics may sometimes decrease the
Treatment Once pancreatic infection is diagnosed, support- severity of pancreatitis,125 and endoscopic cannulation of the
ive measures are initiated, including nasogastric suction, with- pancreatic duct has yielded bacteria in pancreatic secretions of
holding of oral feedings, meticulous attention to respiratory care patients with acute pancreatitis.126 In patients with pancreatic
and fluid and electrolyte balance, systemic antibiotic therapy, and abscess, bacteriologic cultures are usually polymicrobial, the
nutritional support. The key to successful treatment, however, is most common organisms being E. coli, enterococci, Klebsiella
surgical, radiologic, or endoscopic drainage. pneumoniae, P aeruginosa, S. aureus, Bacteroides fragilis, and Clos-
.
Pancreatic necrosis. Sterile pancreatic necrosis alone is not an tridium perfringens. There is a growing trend toward early use of
indication for surgical debridement. In one prospective study, 11 prophylactic antibiotics in cases of pancreatic necrosis, even
patients with sterile pancreatic necrosis were all followed success- though there are no data that convincingly demonstrate a clini-
fully with conservative treatment.117 However, once infected pan- cal benefit. This trend may be partly responsible for the increas-
creatic necrosis is confirmed by Gram stain or culture, surgical ing prevalence of Candida species in pancreatitis-related sepsis; a
debridement is required to remove the characteristically thick 1996 report stated that Candida infection was detected in 21%
necrotic material; radiologic or endoscopic methods alone are not of patients.127
as effective for this purpose. Nutrition. Nutritional support of patients with pancreatic abs-
The choice of drainage technique is nevertheless controversial. cesses usually consists of TPN, though small bowel feeding may
Many clinicians prefer operative debridement and sump drainage. be attempted occasionally.These patients have high metabolic de-
The mortality associated with extensive operative debridement (so- mands and may experience glucose intolerance or hyperlipi-
called necrosectomy) and sump drainage may range from 30% to demia. Nevertheless, they generally tolerate I.V. feeding well. A
40%,118 and this technique may be associated with a 30% to 40% 10-fold increase in mortality (from 2.5% to 21%) was reported
reoperation rate because of sepsis or GI complications.28,119 in patients in whom a positive nitrogen balance could not be
Open drainage. To reduce the frequency of reoperation and to achieved.128
lower mortality, some clinicians opt for open drainage or marsu-
pialization of the infected pancreas. One modification involves the Splenic Abscess
use of a prosthetic mesh and a zipper to facilitate reexploration in Diagnosis A splenic abscess should be considered in patients
patients with severe intra-abdominal abscess.120 A 1991 meta- who present with fever and a left upper quadrant mass, though it
analysis of published surgical studies on infected pancreatic necro- remains a rare cause of these symptoms. Most splenic abscesses
sis found statistically better results with debridement and lavage or encountered in clinical practice are solitary; multiple abscesses are
debridement and open packing than with extensive debridement usually covert and are typically found at autopsy in patients with
and sump drainage.121 However, surgical treatment should be cus- disseminated malignancy, collagen vascular disease, or chronic
tomized for each patient. In one study, open packing was used for debility.
massive necrosis (more than 100 g removed by debridement at Because splenic abscess is rare, correct diagnosis requires a high
operation or CT evidence of at least 50% pancreatic necrosis) or index of suspicion.The main clue is the clinical setting: both bactere-
for extrapancreatic necrosis, whereas conventional debridement mia and local splenic disease are required to produce splenic abscess.
and sump drainage were used in other cases; the overall mortality In the preantibiotic period, this combination was seen most frequent-
in this study was only 14%.122 ly in patients with bacterial endocarditis and typhoid. Even today,
Pancreatic abscess. Pancreatic abscess resulting from liquefaction more than three quarters of splenic abscesses occur in patients who
of necrosis is also best treated by surgical drainage because resid- already have an infection elsewhere in the body; splenic abscesses
ual necrosis may cause failure of treatment by percutaneous meth- can also occur in patients with splenic infarcts, splenic hematomas,
ods.123 On the other hand, infected pancreatic fluid collections and or local splenic disease caused by hemoglobinopathies.](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-12-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 13
a Pancreas b Pancreas
c Pancreas d
Pancreas
Fluid
e Fluid Pancreas f Abscess
Fluid
Figure 7 Pancreatic findings on CT scan have been graded by Ranson into five categories: grade A—normal pancreas
(a); grade B—diffuse enlargement of pancreas and nonhomogeneous density of gland (b); grade C—diffuse enlargement
of pancreas associated with peripancreatic inflammation (c); grade D—high-density fluid collection in left anterior
pararenal space (only head of pancreas is visualized at this level) (d); and grade E—diffuse enlargement of pancreas
with several intrapancreatic small fluid collections and poorly defined fluid collections adjacent to tail and head of pan-
creas (e). In final CT scan (f), pancreatic abscess is demonstrated; partially encapsulated fluid collection containing
bubbles of air represents large abscess.
The diagnosis of splenic abscess may be supported by indirect tion or abdominal CT scan is required. The abdominal CT scan,
radiologic signs, such as an elevated left hemidiaphragm or the enhanced with I.V. or oral contrast material, is preferred [see Figure
finding of a left upper quadrant air-fluid level (mimicking the stom- 8].129 This technique provides a direct image of the spleen, on
ach). To clinch the diagnosis, an abdominal ultrasound examina- which abscesses appear as low-density areas that may contain gas.](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-13-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 14
Mass
Figure 8 Abdominal CT scan, enhanced by contrast material, confirms diagnosis of splenic abscess.
Infections of the Lower Abdomen
Treatment Treatment of splenic abscess includes I.V. admin-
istration of antibiotics and splenectomy [see 5:25 Although enteric perforations, like pancreatitis and cholecystitis,
Splenectomy].The usual pathogenic organisms found are staphylo- present most commonly with pain and fever, their diagnosis differs
cocci and streptococci, though gram-negative bacilli and anaer- from that of upper abdominal infections of the solid organs.The pain
obes may also be present.When splenic abscesses are not drained, associated with enteric perforation frequently is not well localized;
mortality approaches 100%. At one time, splenotomy was the pre- consequently, CT scanning is used more frequently than ultra-
ferred operative treatment, but splenectomy is currently the pre- sonography because it is superior for evaluating the entire abdomen
ferred approach. Percutaneous catheter drainage is being per- [see Figure 9]. Moreover, a perforated viscus may present more acute-
formed with increasing frequency and appears to be as effective as ly than other forms of infection do, and it is a common indication
operative drainage.8,130.131 for emergency exploration. Thus, in the setting of a possible lower
Patient does not have "certain" appendicitis, signs of
upper abdominal infection are not present, and abdominal
plain films are not indicated
Order abdominal and pelvic CT scans.
Diffuse infection is Free peritoneal air is Evidence of duodenal Localized infection
Scans are normal
observed; infection seen without evidence perforation is seen, with or is seen
is uncontrolled, and of controlled leak without free peritoneal air
Consider nonsurgical
source is unclear (duodenal ulcer,
diagnoses. Treat operatively; if upper GI
periappendiceal or
Consider esophago- diverticular abscess) study shows perforation is
Resuscitate, give
gastroduodenoscopy. sealed, consider nonoperative
antibiotics, and take
to OR. Resuscitate, give treatment.
antibiotics, and take
to OR.
No discrete fluid collection is Discrete fluid collection is
present (pancreatitis, present (periappendiceal or
diverticulitis) diverticular abscess)
Provide nonoperative management, Resuscitate and give antibiotics.
including resuscitation and Treatment options:
antibiotic therapy (antibiotics are • percutaneous drainage with
unnecessary for bland pancreatitis delayed resection
Figure 9 Algorithm outlines approach to patient with without necrosis). • immediate open resection and
suspected lower abdominal infection. drainage
• diversion and drainage only](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-14-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 15
a b
c
Figure 10 (a) Upright chest x-ray of patient with
sudden onset of diffuse abdominal pain demonstrates
free peritoneal air underneath both diaphragms
(black arrows). Emergency exploration was carried
out without further studies, and perforated gastric
ulcer was excised. (b) Abdominal CT scan of patient
with history of ulcer disease and 1-week history of
increasing abdominal pain shows retrogastric fluid
collection with air that appears to be in communica-
tion with duodenum (white arrow). Patient under-
went laparotomy, and perforated duodenal ulcer was
repaired. (c) Abdominal CT scan of patient with 2- to
3-day history of worsening abdominal pain demon-
strates extravasation of oral contrast from anterolat-
eral aspect of duodenum (white arrow). Patient
underwent laparoscopic omental patch closure.
abdominal infection, the diagnostic emphasis is on confirming or a role for H. pylori infection in the pathogenesis of these perfora-
ruling out the presence of an acute condition necessitating opera- tions as well.136
tion, rather than on fine localization of a more chronic illness.
Diagnosis
PEPTIC ULCER PERFORATION
A patient with a perforated peptic ulcer will complain of the
The incidence of peptic ulcer perforation has decreased signifi- sudden onset of intense abdominal pain and will often be able to
cantly as a consequence of the changes in disease progression and pinpoint the exact time when the symptoms began. If the perfora-
incidence of intractable ulcers brought about by the advent of H2 tion has not spontaneously sealed or been managed with operative
receptor antagonists and proton pump inhibitors (PPIs). Still, a closure, the clinical picture can progress to florid sepsis and shock.
significant percentage of all hospital admissions are secondary to Evidence of free air on plain upright and left lateral decubitus radi-
perforated peptic ulcers, and the patient population is becoming ographs will be seen in as many as 70% of cases [see Figure 10a].137
older and more evenly balanced between men and women, pre- Endoscopy should be avoided in the evaluation of peptic ulcer per-
sumably because of increased use of nonsteroidal anti-inflamma- foration, but equivocal cases or spontaneously sealed perforations
tory drugs and cigarettes.132 can be evaluated with water-soluble contrast studies. CT scanning
Several studies found a high (80% to 92%) incidence of can be used to localize an infection to the duodenum, particular-
Helicobacter pylori infection in patients with perforated peptic ly if communication of air or fluid with the duodenum is estab-
ulcers.133,134 Although the prevalence of H. pylori infection in this lished [see Figure 10b] or if extravasation of contrast is seen [see
population is well established, the causal role that such infection Figure 10c].
plays in peptic ulcer perforations has been questioned.135 In a 1999
study involving 50 patients with juxtapyloric perforations related to Treatment
crack cocaine use who were successfully managed with simple Surgical management centers on control of the site of perfora-
omental patch closure, the investigators found that approximately tion (via surgical closure or spontaneous sealing), with or without
80% of the patients who underwent antral mucosal biopsy at the an acid-reducing procedure [see 5:20 Gastric Duodenal Disease]. Be-
time of closure had a positive urease test, a finding that suggested fore this is done, I.V. fluids should be given, metabolic derange-](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-15-2048.jpg)

![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 17
[see 5:29 Intestinal Anastomosis]. For patients with Crohn disease,
perforation (usually presenting as a fistula) is a risk factor for post-
operative disease recurrence156; accordingly, close postoperative
follow-up is indicated.
There are two additional issues regarding small bowel perfora-
tions that warrant special mention. The first has to do with small
bowel perforation secondary to obstruction. When this event
occurs, it is important not only that the perforated segment be
resected but also that the cause of obstruction be identified to pre-
vent recurrence. The second issue has to do with anastomotic
leakage. Not all leaks call for surgical intervention. If the leak is a
late complication, it is likely to have walled itself off into an
abscess, in which case CT-guided drainage of the abscess is the
treatment of choice. Efforts at reducing the luminal transport are
also made to improve healing.
Nutritional support plays a major supportive role in the treat-
ment of patients with small bowel perforation. Many of these
patients, either because of their underlying pathology (e.g., Crohn
disease) or because of their hypermetabolic state (e.g., from trau-
ma), lose some of their innate ability to heal and prevent anasto-
motic breakdown.The presence of a knowledgeable nutrition staff
can dramatically enhance patient recovery in this setting. Figure 11 Pelvic CT scan of patient with distant history of right
lower quadrant abdominal pain with recurrent acute attack
demonstrates inflamed and thickened appendix with surrounding
Antibiotic therapy The small bowel flora is typically sparse
fat stranding (white arrow). Gangrenous appendix was removed
(103 to 104/ml), with salivary organisms predominating. In condi- laparoscopically.
tions of stasis, obstruction, or impaired motility, however, colonic
flora can proliferate, with E. coli, enterococci, and obligate anaer-
obes the dominant organisms. In the distal ileum, there are typi- from 39% to 8%, and one retrospective study found that the use
cally about 106 colony-forming units/ml, with an increasing pro- of diagnostic CT lowered the rate of misdiagnosis to 7%.162 CT
portion of enteric organisms and anaerobic bacteria, presumably scanning is reported to be 93% to 98% in diagnosing appendici-
as a result of backwash through the ileocecal valve.157 Although tis, with significantly improved accuracy achieved by using an
there are generally far fewer bacteria in the small intestine than in appendicitis protocol after retrograde water-soluble contrast
the colon (which contains about 1012 organisms/ml), the standard administration.163 CT findings suggestive of appendicitis [see
antimicrobial therapy remains broad-spectrum coverage (e.g., flu- Figure 11] include enlargement and dilation of the appendix (to
oroquinolone plus an antianaerobic agent for 5 days).158 > 6 mm), nonfilling of the appendix, and periappendiceal inflam-
mation (fat stranding, abscess, phlegmon, and dependent fluid
APPENDICITIS collections); these findings do not differ significantly between
Obstruction of the appendiceal lumen by a fecalith, a hyper- acute appendicitis and chronic, recurrent appendicitis.164,165
plastic lymph node, or a foreign body is typically the inciting event Current evidence supports the role of CT scanning in the diag-
in the pathogenesis of appendicitis. Luminal obstruction with con- nostic evaluation of patients with suspected appendicitis. Studies
tinued secretion results in progressive distention, proliferation of have demonstrated decreases both in the incidence of normal
luminal microorganisms, ischemia, gangrene, and subsequent per- appendectomies and in the incidence of prolonged, unnecessary
foration. The clinical history during this evolution is marked by observations.166,167 Furthermore, alterations in patient manage-
diffuse epigastric pain with anorexia, nausea, and vomiting. The ment attributable to diagnostic CT have been shown to decrease
pain typically progresses first to the periumbilical region and then overall hospital and patient costs. Nevertheless, the utility of CT in
to the right lower quadrant (at McBurney’s point). Patients have a young men whose history, physical examination, and laboratory
low-grade fever and exhibit direct tenderness at McBurney’s point test results fit the classic picture of appendicitis remains unproven;
but may also manifest rebound tenderness, guarding, rigidity, and this subset of patients may be managed without confirmatory
marked temperature elevation if the appendix perforates and CT.166 On the other hand, CT scanning appears to be quite useful
results in diffuse peritonitis. As the viscera and the omentum local- for diagnosing appendicitis in women, in which setting it decreases
ize and sequester the perforation, the symptoms may subside to a the incidence of normal appendectomies and facilitates diagnosis
degree, with localized pain and a palpable abdominal mass the pri- of other causes of the symptoms.168,169 Preoperative CT scanning
mary manifestations remaining. assists in planning an operation, identifying a periappendiceal
abscess that may delay immediate appendectomy, and recognizing
Diagnosis other sources of intra-abdominal pathology.
Classically, the diagnosis of appendicitis has been made pri-
marily through clinical examination, with laboratory tests consis- Treatment
tent with inflammation (i.e., an elevated leukocyte count with a Initial management consists of fluid resuscitation, appropriate
left shift and an elevated C-reactive protein level) serving as con- prophylactic antibiotics, and preparation for surgery. Currently,
firmation. In as many as 20% of patients with appendicitis, how- acute nonperforated appendicitis, gangrenous appendicitis, and
ever, the incorrect diagnosis is made, and the incidence of removal perforated appendicitis without an associated abscess are man-
of a normal appendix can approach 40%.159-161 Early diagnosis of aged with urgent appendectomy [see 5:26 Appendectomy]. The
appendicitis can decrease the risk of postoperative complications main dilemmas in management center on the appropriate use of](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-17-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 18
laparoscopic appendectomy and the role of conservative manage- currence and progression to chronic appendicitis supports the use
ment for periappendiceal masses with interval appendectomy. of interval appendectomy in young patients, but in adults, the de-
cision algorithm must also consider the incidental diagnosis of tumor.
Laparoscopic versus open appendectomy In several Interval appendectomy is typically performed between 6 weeks
prospective, randomized clinical trials that compared laparoscop- and 3 months after percutaneous intervention and clinical resolu-
ic with open appendectomy, the consensus was that the former tion [see Figure 12]. The risk of recurrence is greatest after the 6-
was associated with a lower incidence of wound infection, month point in the clinical progression of acute appendicitis man-
decreased utilization of pain medication, earlier return to normal aged conservatively.183 In several retrospective analyses, interval
activities, and reduced cost of hospitalization (though the data appendectomy proved to be a safe management plan, but to date,
were conflicting on this last point).170-173 On the other hand, the there have been no randomized, prospective trials evaluating its
trials found the laparoscopic approach to be associated with sig- role in management.184,185
nificantly longer operating time, equivalent duration of hospital-
ization, and a possible increased risk of abscess formation. A ret- Antibiotic therapy The pathogenic organisms recovered in
rospective review published in 2000, however, found that when a peritoneal cultures derive from the colon and consist of aerobic or
dedicated laparoscopic service was established for patients with facultative bacteria and anaerobes. The most frequently isolated
appendicitis, the rates of intra-abdominal abscess formation after organisms are E. coli, enterococci, viridans streptococci, B. fragilis,
laparoscopic appendectomy decreased to levels equivalent to those Lactobacillus species, Prevotella melaninogenica, and Bilophila
reported after open appendectomy.174 wadsworthia.186,187 It is noteworthy that the use of intraoperative
Although laparoscopic appendectomy is associated with a high- peritoneal cultures has not been shown to affect the incidence of
er incidence of intra-abdominal abscess formation in the setting of wound infection, abscess formation, or small bowel obstruction if
perforated appendicitis, it is not associated with a higher incidence patients are presumptively managed with antibiotics that cover
of wound infection or abscess in patients with gangrenous or non- gram-negative bacteria and enteric anaerobes.188
perforated appendicitis.175 Furthermore, a prospective, random- Appropriate coverage can be obtained with any of the following:
ized trial found that laparoscopic appendectomy was associated ampicillin-sulbactam, piperacillin-tazobactam, ticarcillin-clavu-
with reduced overall cost of hospitalization, decreased use of pain lanate, cefoxitin, cefotetan, and ciprofloxacin plus metronida-
medication, and earlier return to functional status in patients with zole.189-192 In a trial involving children with perforated appendici-
uncomplicated appendicitis.170 tis, conversion to oral therapy after parenteral therapy was equiv-
Two groups of patients clearly benefit from laparoscopic appen- alent to parenteral therapy alone.193 In a study of patients with
dectomy: women and obese patients. In women, laparoscopy aids acute nonperforated appendicitis, preoperative administration of
in the diagnosis of other pelvic pathologic conditions and lowers cefoxitin was superior to placebo in reducing the incidence of
the incidence of negative appendectomies; in obese patients, it wound infection.190 In a study of children with acute nonperforat-
results in less postoperative pain and a shorter recovery time, even ed appendicitis, prolonged antibiotic administration (5 days) had
though it does not significantly reduce the postoperative compli- no advantage over a single preoperative dose with respect to the
cation rate.176,177 Patients who present with evidence of perforated incidence of wound infection or subsequent abscess formation.194
or complicated appendicitis may be better managed with the tra- The duration and timing of antibiotic administration in patients
ditional open approach to minimize the risk of postoperative with nonperforated gangrenous appendicitis have not been shown
abscess formation.178 Improvements in laparoscopic techniques, to correlate with the wound infection rate.195
however, may eventually reduce the incidence of this complication
COLONIC PERFORATION
to a level comparable to that seen with open management.
Periappendiceal abscess and interval appendectomy Diagnosis
The mainstays of conservative management have been parenteral Diagnostic strategies for identifying colon lesions associated
antibiotics, supportive fluid resuscitation, and percutaneous with intra-abdominal infection follow the general approach out-
drainage of radiographically amenable fluid collections. In a 2001 lined earlier [see Clinical Evaluation and Investigative Studies,
review of 155 patients with periappendiceal abscesses, the compli- above]. For unstable patients with generalized peritonitis, there is
cation rate was 36% for patients managed with surgical incision no need to delay operative intervention to wait for radiologic con-
and drainage and appendectomy, compared with 17% for patients firmation: the pathologic condition will be identified in the course
managed nonoperatively.179 The recurrence rate was 8% in the of the operation. However, for patients who have localized peri-
conservatively managed patients, and nonoperative management tonitis or those who are stable and whose physical examination is
failed in five patients. Patients with perforated appendicitis and not conclusive for peritonitis, radiologic evaluation is pivotal in
abscess or phlegmon diagnosed by CT scanning but without a planning treatment.
palpable mass were safely managed with conservative therapy. In Although plain films may reveal free air in the abdomen and
a 2002 study, immediate appendectomy was associated with a prompt surgical intervention, CT scanning may be a more valu-
higher postoperative complication rate and an increased incidence able first study because of its ability to delineate the bowel wall and
of more extensive initial operations (e.g., ileocecal resection, right surrounding soft tissues with remarkable accuracy. In a 2002
hemicolectomy, and temporary ileostomy).180 study comparing abdominal radiography with CT for the evalua-
The recurrence rate after conservative management ranges tion of acute nontraumatic abdominal pain in the ED, the former
from 10% to 20%. In one study of patients managed with interval was not nearly as diagnostically sensitive as the latter (a nonspe-
appendectomy for periappendiceal mass, histologic evaluation cific diagnosis in 68%, compared with a specific diagnosis in
revealed that a significant majority of samples had a patent appen- 80%).196 The investigators concluded that CT was the initial radi-
diceal lumen and were at risk for recurrent appendicitis.181 In a ographic modality of choice for patients with acute abdominal
2002 report, 45.8% of interval appendectomy pathologic samples pain in the ED. Another study found that CT scans frequently
showed evidence of chronic active inflammation.182 The risk of re- changed physicians’ initial diagnoses, increased diagnostic certain-](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-18-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 19
a b
Figure 12 (a) Pelvic CT scan of young patient with a 5-day history of right lower quadrant abdominal
pain shows fluid collection containing air adjacent to appendix and consistent with appendiceal perfora-
tion and abscess formation (white arrow). (b) Pelvic CT scan of same patient after percutaneous ultra-
sound-guided placement of drainage catheter shows evacuation of air and much fluid. Patient underwent
uneventful interval appendectomy 6 weeks later.
ty, and led to more appropriate treatment in patients with acute management, including broad-spectrum antibiotics and bowel
abdominal pain in the ED.197 rest.The patient can be evaluated for definitive surgical treatment
In view of the relatively high cost of CT scanning, the con- later, after the episode resolves and the patient is in better condi-
comitant radiation exposure, and the use of I.V. contrast agents to tion for surgery. For larger abscesses or stage II disease [see Figure
enhance the scans, some have suggested using ultrasonography to 13b], the standard of care is CT-guided percutaneous abscess
make diagnoses. However, the well-documented dependency of drainage, if feasible. After drainage, resuscitation, and bowel prep-
this modality on the skill of the individual technician makes it less aration, a one-stage colectomy can be done (resection of the dis-
attractive to the broader health care community, where full-time eased segment with primary anastomosis) so as to avoid the poten-
sonographers are not always available. Finally, it should be noted tial increased morbidity of a two-stage procedure.205
that there is no role for MRI in the acute setting. Although it is For patients who have abscesses that are inaccessible to percu-
both sensitive and specific, the logistic hindrances associated with taneous drainage or who experience persistent symptoms despite
its use greatly limit its applicability. drainage, operative correction is required. If adequate bowel pre-
paration can be carried out, primary anastomosis at the time of
Treatment surgery should be considered. If adequate bowel preparation is not
Diverticulitis Diverticular disease ranges in severity from possible, a two-stage approach, including a Hartmann procedure
minor to serious. The focus of our discussion will be on manage- and subsequent stoma reversal, should be considered. Alterna-
ment of complicated (perforated) diverticular disease, for which tively, depending on the patient’s condition, resection with prima-
resection should be considered after only one attack. ry anastomosis may be attempted. There is some evidence that
In the past, treatment of perforated diverticular disease involved a employing intraoperative colonic lavage to reduce the fecal col-
multistage surgical approach whereby the patient underwent three umn and thus allow primary anastomosis may reduce morbidity,
separate procedures: one for fecal diversion and drainage of the especially in patients with stage I or II disease.206-208 However, the
infection, a second for resection of the diseased segment, and a third studies supporting this view are not conclusive enough for such a
for closure of the colostomy.This three-stage approach proved to be regimen to be considered standard; further investigation is war-
associated with high morbidities, high cumulative mortalities, and ranted before it is generally accepted. Finally, whether to add a
prolonged hospitalizations.198-200 Since then, CT -guided percuta- covering stoma to a primary anastomosis is a case-by-case decision
neous drainage, primary resection of the diseased segment, and that is usually guided by the presence of risk factors such as poor
improved patient selection for resection and primary anastomosis nutritional status, inadequate bowel preparation, blood loss, or
have improved patient outcomes dramatically. Few adequately pow- intraoperative hypotension.209
ered multicenter, prospective, randomized trials evaluating treat-
ment of complicated diverticular disease have been done; accord-
ingly, many of the current treatment standards have been derived by
consensus on the basis of thorough review of the literature. Table 4—Hinchey System for Classification
Therapy for perforated diverticular disease depends greatly on of Perforated Diverticulitis201
the patient’s condition at the time of presentation and on the stage
of the disease.The Hinchey staging system201 [see Table 4] classifies Stage Description
perforated diverticular disease according to the associated inflam-
Stage I Pericolic or mesenteric abscess
matory process and is used to guide and compare treatment
Stage II Pelvic or retroperitoneal abscess that is walled off
options.202-204
Stage III Purulent peritonitis
In stage I disease, a small pericolic abscess [see Figure 13a] in a Stage IV Feculent peritonitis
stable and otherwise healthy patient may resolve with conservative](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-19-2048.jpg)

![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 21
a b
Figure 14 (a) Abdominal CT scan of elderly patient with history of vascular disease and worsening
abdominal pain over a 3-day period shows diffuse inflammation and right upper quadrant extraluminal
air (white arrow). Patient underwent emergency exploration, and ischemic perforation of cecum was
found. Right hemicolectomy and temporary diverting ileostomy were performed. (b) Abdominal CT
scan of patient with history of Crohn disease and worsening abdominal pain demonstrates thickening of
colonic wall with both intramural and extramural air (white arrow). Patient was treated with emergency
total abdominal colectomy for pancolitis with creation of temporary diverting ileostomy.
dures.Two studies from the early 1990s suggested improved long- [see Table 5] that cannot be attributed to another cause.To reduce
term mortality after primary resection.226,227 A subsequent study, undue treatment-associated morbidity, additional criteria are sup-
however, suggested that the improved mortality associated with plied to aid in specifying precisely who should receive treatment.
primary resection was secondary to preselection and therefore Treatment of PID, according to the CDC, includes broad-spec-
could not be considered conclusive proof of the superiority of this trum antibiotics directed toward Neisseria gonorrhoeae, Chlamydia
approach.The authors of this latter study concluded that primary trachomatis, anaerobes, gram-negative facultative bacteria, and
resection was appropriate for a select patient population with min- streptococci [see Table 6]. Hospitalization is suggested when surgi-
imal comorbidity and that staged resection was beneficial for cal emergencies (e.g., appendicitis) cannot be excluded or when
patients with a high degree of acute illness and comorbidity (e.g., the patient is pregnant; does not respond clinically to oral antimi-
elderly patients).228 crobial therapy; cannot follow or tolerate an outpatient oral regi-
Less common causes of colonic perforation. Other diagnoses associ- men; has severe illness, nausea and vomiting, or high fever; or has
ated with colonic perforation and peritonitis (localized or diffuse) a tubo-ovarian abscess. Surgical intervention for PID is generally
are ischemic necrosis as a result of vasculopathology [see Figure limited to patients with symptomatic pelvic masses, ruptured
14a] or volvulus, missed traumatic injury, and IBD [see Figure 14b].
Except for IBD, the standard therapy is excision of the affected seg-
ment and reanastomosis, with or without a covering stoma. For
patients with numerous comorbidities, a high degree of feculent Table 5—CDC Guidelines for Diagnosis of
contamination, or very severe illness necessitating an extremely
abbreviated operating time, a Hartmann procedure with a mucous
Pelvic Inflammatory Disease230
fistula or an oversewn distal segment is the primary treatment. Minimal symptoms
Because perforation associated with IBD is typically a self-limited Uterine/adnexal tenderness
disease, treatment is directed at the underlying pathophysiology Cervical motion tenderness
and excision of the diseased segment is not always indicated.229 Additional supportive criteria (enhance specificity of minimal symptoms)
Oral temperature >101° F (> 38.3° C)
Abnormal cervical or vaginal mucopurulent discharge
Other Abdominal Infections Presence of white blood cells on saline microscopy of vaginal
secretions
PELVIC INFLAMMATORY DISEASE Elevated erythrocyte sedimentation rate
Elevated C-reactive protein
Because of the diverse clinical presentations of pelvic inflam- Laboratory documentation of cervical infection with Neisseria gonorrhoeae
matory disease (PID) and the significant sequelae associated with or Chlamydia trachomatis
delayed diagnosis, women with this condition can pose a major Most specific criteria
diagnostic dilemma in the ED. In 2002, the Centers for Disease Endometrial biopsy with histopathologic evidence of endometritis
Control and Prevention (CDC) updated their established diag- Transvaginal sonography or magnetic resonance imaging techniques
nostic guidelines for initiating therapy in patients with suspected showing thickened, fluid-filled tubes with or without free pelvic fluid or
PID.230 According to these guidelines, empirical treatment should tubo-ovarian complex
Laparoscopic abnormalities consistent with PID
be started if a young sexually active woman or any woman at risk
for sexually transmitted diseases presents with minimal symptoms](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-21-2048.jpg)



![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 25
approach works because of the liver’s luxurious dual blood supply. response to the original insult. Such deaths are still attributed to
On the other hand, multiple peritoneal fluid collections (with- overwhelming sepsis, to multiple organ dysfunction syndrome, or
out a natural blood supply) are not infrequently seen even after to any number of other terms used to describe an irreversible
successful management of diffuse or fecal peritonitis yet can occa- sequence of organ failure and death [see 8:13 Multiple Organ
sionally be managed without drainage. Even if these collections Dysfunction Syndrome].
are subsequently proved to be infected, they may be too numer- Multiple attempts over the years to alter this downward trajec-
ous to approach percutaneously, and ongoing inflammation of the tory by using novel therapies to target this generalized inflamma-
bowel may render an operative approach unsafe. Again, drainage tory response proved unsuccessful. In the past few years, however,
of the largest accessible collection to establish a diagnosis and both recombinant human activated protein C and corticosteroid
guide antibiotic management, followed by long-term antibiotic replacement therapy (for those with sepsis-associated adrenal
therapy, is the most feasible course. In this case, sampling is imper- insufficiency) were shown to improve survival in randomized,
ative because a hospital-acquired intra-abdominal infection is placebo-controlled trials involving mixed populations of patients
more likely to involve less common but more resistant pathogens, with sepsis. Although the number of patients with intra-abdomi-
including fungi. Regardless of the situation, though, the optimal nal infection was relatively small in each study, there was no indi-
duration of antibiotic therapy for small undrained abscesses cation that these agents would not be similarly effective in this spe-
remains to be established. cific subgroup. The overall benefit of each of these treatments
appears to be small, but the results of these trials are highly
ADJUNCTIVE MEDICAL THERAPIES
encouraging in that they suggest that related agents might be able
Until recently, it could be said that advances in surgical therapy to achieve further decreases in mortality.These possibilities, com-
for intra-abdominal infection were outpacing other aspects of bined with significant improvements in general critical care, por-
patient management. Too often, operations were technically suc- tend a future in which significant reductions in mortality may be
cessful, yet patients died afterward as a result of their systemic realized even in the most severely infected patients.
References
1. Schofield PF, Hulton NR, Baildam AD: Is it 14. Windsor AC, Kanwar S, Li AG, et al: Compared 25. Fan ST, Lai EC, Mok FP, et al: Early treatment
acute cholecystitis? Ann R Coll Surg Engl 68:14, with parenteral nutrition, enteral feeding attenu- of acute biliary pancreatitis by endoscopic papil-
1986 ates the acute phase response and improves dis- lotomy. N Engl J Med 328:228, 1993
2. Ranson JH: Acute pancreatitis. Curr Probl Surg ease severity in acute pancreatitis. Gut 42:431, 26. Williamson RC: Early assessment of severity in
16:1, 1979 1998
acute pancreatitis. Gut 25:1331, 1984
3. Winslet M, Hall C, London NJ, et al: Relation of 15. Chatzicostas C, Roussomoustakaki M, Vardas
27. Srinathan SK, Barkun JS, Mehta SN, et al: The
diagnostic serum amylase levels to aetiology and E, et al: Balthazar computed tomography se-
management of gallstone pancreatitis in the lap-
severity of acute pancreatitis. Gut 33:982, 1992 verity index is superior to Ranson criteria and
aroscopic era. J Gastrointest Surg (in press)
APACHE II and III scoring systems in predict-
4. Patti M, Pellegrini CA, Way LW: Serum amylase ing acute pancreatitis outcome. J Clin Gastro- 28. Ranson JH, Spencer FC: Prevention, diagnosis,
is useful in the differential diagnosis of acute enterol 36:253, 2003 and treatment of pancreatic abscess. Surgery
abdominal pain. Gastroenterology 90:1580, 82:99, 1977
16. Liu TH, Kwong KL, Tamm EP, et al: Acute pan-
1986
creatitis in intensive care unit patients: value of 29. Osborne DH, Imrie CW, Carter DC: Biliary
5. Yadav D, Agarwal N, Pitchumoni CS: A critical clinical and radiologic prognosticators at predict- surgery in the same admission for gallstone-asso-
evaluation of laboratory tests in acute pancreati- ing clinical course and outcome. Crit Care Med ciated acute pancreatitis. Br J Surg 68:758, 1981
tis. Am J Gastroenterol 97:1309, 2002 31:1026, 2003 30. Folsch UR, Nitsche R, Ludtke R, et al: Early
6. Smotkin J, Tenner S: Laboratory diagnostic tests 17. Stone HH, Fabian TC, Dunlop WE: Gallstone ERCP and papillotomy compared with conserv-
in acute pancreatitis. J Clin Gastroenterol 34: pancreatitis: biliary tract pathology in relation to ative treatment for acute biliary pancreatitis. The
459, 2002 time of operation. Ann Surg 194:305, 1981 German Study Group on Acute Biliary Pan-
7. Toosie K, Chang L, Renslo R, et al: Early com- 18. Acosta JM, Rossi R, Galli OM, et al: Early creatitis. N Engl J Med 336:237, 1997
puted tomography is rarely necessary in gallstone surgery for acute gallstone pancreatitis: evalua- 31. Chang L, Lo S, Stabile BE, et al: Preoperative
pancreatitis. Am Surg 63:904, 1997 tion of a systematic approach. Surgery 83:367, versus postoperative endoscopic retrograde
8. Sarr MG, Sanfey H, Cameron JL: Prospective, 1978 cholangiopancreatography in mild to moderate
randomized trial of nasogastric suction in 19. Kelly TR: Gallstone pancreatitis: the timing of gallstone pancreatitis: a prospective randomized
patients with acute pancreatitis. Surgery 100: surgery. Surgery 88:345, 1980 trial. Ann Surg 231:82, 2000
500, 1986 32. Nitsche R, Folsch UR, Ludtke R, et al: Urgent
20. Dixon JA, Hillam JD: Surgical treatment of bil-
9. Bradley EL 3rd: Antibiotics in acute pancreatitis: iary tract disease associated with acute pancre- ERCP in all cases of acute biliary pancreatitis? A
current status and future directions. Am J Surg atitis. Am J Surg 120:371, 1970 prospective randomized multicenter study. Eur J
158:472, 1989 Med Res 1:127, 1995
21. Ranson JH:The timing of biliary surgery in acute
10. Steinberg WM, Schlesselman SE: Treatment of pancreatitis. Ann Surg 189:654, 1979 33. Kozarek RA, Patterson DJ, Ball TJ, et al:
acute pancreatitis: comparison of animal and Endoscopic placement of pancreatic stents and
22. Paloyan D, Simonowitz D, Skinner DB:The tim-
human studies. Gastroenterology 93:1420, 1987 drains in the management of pancreatitis. Ann
ing of biliary tract operations in patients with
Surg 209:261, 1989
11. McArdle AH, Rosenberg M, Fried GM, et al: pancreatitis associated with gallstones. Surg
Pancreatic exocrine secretion in response to con- Gynecol Obstet 141:737, 1975 34. Ranson JH, Berman RS: Long peritoneal lavage
tinuous and bolus feeding (abstract), 19th Annu- decreases pancreatic sepsis in acute pancreatitis.
23. Kelly TR, Wagner DS: Gallstone pancreatitis: a
al Meeting, Association for Academic Surgery, Ann Surg 211:708, 1990
prospective randomized trial of the timing of
Cincinnati, Ohio, 1985 surgery. Surgery 104:600, 1988 35. Pederzoli P, Bassi C, Vesentini S, et al: A ran-
12. Erstad BL: Enteral nutrition support in acute domized multicenter clinical trial of antibiotic
24. Neoptolemos JP, Carr-Locke DL, London NJ, et
pancreatitis. Ann Pharmacother 34:514, 2000 prophylaxis of septic complications in acute nec-
al: Controlled trial of urgent endoscopic retro-
13. Scolapio JS, Malhi-Chowla N, Ukleja A: Nutri- grade cholangiopancreatography and endoscopic rotizing pancreatitis with imipenem. Surg Gyn-
tion supplementation in patients with acute and sphincterotomy versus conservative treatment ecol Obstet 176:480, 1993
chronic pancreatitis. Gastroenterol Clin North for acute pancreatitis due to gallstones. Lancet 36. Luiten EJ, Hop WC, Lange JF, et al: Controlled
Am 28:695, 1999 2:979, 1988 clinical trial of selective decontamination for the](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-25-2048.jpg)
![© 2004 WebMD Inc. All rights reserved. ACS Surgery: Principles and Practice
8 CRITICAL CARE 18 Intra-Abdominal Infection — 26
treatment of severe acute pancreatitis. Ann Surg Prophylactic antibiotics for elective laparoscopic 77. Leung JW, Chung SC, Sung JJ, et al: Urgent en-
222:57, 1995 cholecystectomy: are they necessary? Arch Surg doscopic drainage for acute suppurative cho-
37. Sharma VK, Howden CW: Prophylactic antibiot- 134:611, 1999 langitis. Lancet 1:1307, 1989
ic administration reduces sepsis and mortality in 58. Illig KA, Schmidt E, Cavanaugh J, et al: Are pro- 78. Lomanto D, Pavone P, Laghi A, et al: Magnetic
acute necrotizing pancreatitis: a meta-analysis. phylactic antibiotics required for elective laparo- resonance-cholangiopancreatography in the diag-
Pancreas 22:28, 2001 scopic cholecystectomy? J Am Coll Surg 184: nosis of biliopancreatic diseases. Am J Surg
38. Golub R, Siddiqi F, Pohl D: Role of antibiotics in 353, 1997 174:33, 1997
acute pancreatitis: a meta-analysis. J Gastrointest 59. Karachalios GN, Nasiopoulou DD, Bourlinou PK, 79. Becker CD, Grossholz M, Mentha G, et al: MR
Surg 2:496, 1998 et al:Treatment of acute biliary tract infections with cholangiopancreatography: technique, potential
39. Uhl W, Warshaw A, Imrie C, et al: IAP Guide- ofloxacin: a randomized, controlled clinical trial. Int indications, and diagnostic features of benign,
lines for the Surgical Management of Acute Pan- J Clin Pharmacol Ther 34:555, 1996 postoperative, and malignant conditions. Eur
creatitis. Pancreatology 2:565, 2002 60. Krajden S,Yaman M, Fuksa M, et al: Piperacillin Radiol 7:865, 1997
40. Howard TJ, Temple MB: Prophylactic antibiotics versus cefazolin given perioperatively to high-risk 80. Gigot JF, Leese T, Dereme T, et al: Acute cholan-
alter the bacteriology of infected necrosis in patients who undergo open cholecystectomy: a gitis: multivariate analysis of risk factors. Ann
severe acute pancreatitis. J Am Coll Surg 195: double-blind, randomized trial. Can J Surg 36: Surg 209:435, 1989
759, 2002 245, 1993 81. Lai EC, Tam PC, Paterson IA, et al: Emergency
41. Fiedler F, Jauernig G, Keim V, et al: Octreotide 61. Skillings JC, Kumai C, Hinshaw JR: Cholecys- surgery for severe acute cholangitis: the high-risk
treatment in patients with necrotizing pancreati- tostomy: a place in modern biliary surgery? Am patients. Ann Surg 211:55, 1990
tis and pulmonary failure. Intensive Care Med J Surg 139:865, 1980 82. O’Connor MJ, Schwartz ML, McQuarrie DG, et
22:909, 1996 62. Klimberg S, Hawkins I, Vogel SB: Percutaneous al: Acute bacterial cholangitis: an analysis of clin-
42. Paran H, Neufeld D, Mayo A, et al: Preliminary cholecystostomy for acute cholecystitis in high- ical manifestation. Arch Surg 117:437, 1982
report of a prospective randomized study of risk patients. Am J Surg 153:125, 1987 83. Thompson JE Jr, Tompkins RK, Longmire WP
octreotide in the treatment of severe acute pan- 63. Miyazaki K, Uchiyama A, Nakayama F: New Jr: Factors in management of acute cholangitis.
creatitis. J Am Coll Surg 181:121, 1995 approach to the timing of operative intervention Ann Surg 195:137, 1982
43. de Souza LJ, Sampietre SN, Assis RS, et al: for acute cholecystitis: use of ultrasound risk 84. Bismuth H, Kuntziger H, Corlette MB: Cho-
Effect of platelet-activating factor antagonists score (abstr). 32nd World Conference of Sur- langitis with acute renal failure: priorities in ther-
(BN-52021, WEB-2170, and BB-882) on bacte- gery, Sydney, Australia, September 20–26, 1987 apeutics. Ann Surg 181:881, 1975
rial translocation in acute pancreatitis. J Gas- 64. England RE, McDermott VG, Smith TP, et al: 85. Cho SR, Turner MA: Hepatic abscesses due to
trointest Surg 5:364, 2001 Percutaneous cholecystostomy: who responds? suppurative cholangitis. South Med J 75:488,
44. Lane JS, Todd KE, Gloor B, et al: Platelet acti- AJR Am J Roentgenol 168:1247, 1997 1982
vating factor antagonism reduces the systemic 65. Orlando R 3rd, Crowell KL: Laparoscopy in the 86. Gould RJ, Vogelzang RL, Neiman HL, et al:
inflammatory response in a murine model of critically ill. Surg Endosc 11:1072, 1997 Percutaneous biliary drainage as an initial thera-
acute pancreatitis. J Surg Res 99:365, 2001
66. Reynolds BM, Dargan EL: Acute obstructive py in sepsis of the biliary tract. Surg Gynecol
45. Kingsnorth AN, Galloway SW, Formela LJ: cholangitis: a distinct clinical syndrome. Ann Obstet 160:523, 1985
Randomized, double-blind phase II trial of Surg 150:299, 1959 87. Leese T, Neoptolemos JP, Baker AR, et al: Man-
lexipafant, a platelet-activating factor antagonist,
67. Baer HU, Matthews JB, Schweizer WP, et al: agement of acute cholangitis and the impact of
in human acute pancreatitis. Br J Surg 82:1414,
Management of the Mirizzi syndrome and the endoscopic sphincterotomy. Br J Surg 73:988,
1995
surgical implications of cholecystcholedochal fis- 1986
46. Johnson CD, Kingsnorth AN, Imrie CW, et al: tula. Br J Surg 77:743, 1990 88. Davis AJ, Kolios G, Alveyn CG, et al: Antibiotic
Double blind, randomised, placebo controlled
68. Textor HJ, Flacke S, Pauleit D, et al: Three- prophylaxis for ERCP: a comparison of oral
study of a platelet activating factor antagonist,
dimensional magnetic resonance cholangiopan- ciprofloxacin with intravenous cephazolin in the
lexipafant, in the treatment and prevention of
organ failure in predicted severe acute pancreati- creatography with respiratory triggering in the prophylaxis of high-risk patients. Aliment Phar-
tis. Gut 48:62, 2001 diagnosis of primary sclerosing cholangitis: com- macol Ther 12:207, 1998
parison with endoscopic retrograde cholangiog- 89. Saini S: Imaging of the hepatobiliary tract. N
47. Mentzer RM Jr, Golden GT, Chandler JG, et al: raphy. Endoscopy 34:984, 2002
A comparative appraisal of emphysematous cho- Engl J Med 336:1889, 1997
lecystitis. Am J Surg 129:10, 1975 69. Ferrara C, Valeri G, Salvolini L, et al: Magnetic 90. Bearcroft PW, Miles KA: Leucocyte scintigraphy
resonance cholangiopancreatography in primary or computed tomography for the febrile post-
48. Turner RJ 3rd, Becker WF, Coleman WO, et al:
sclerosing cholangitis in children. Pediatr Radiol operative patient? Eur J Radiol 23:126, 1996
Acute cholecystitis in the diabetic. South Med J
32:413, 2002
62:228, 1969 91. Haque R, Ali IK, Akther S, et al: Comparison of
70. Chen JH, Chai JW, Chu WC, et al: Free breath- PCR, isoenzyme analysis, and antigen detection
49. Turrill RL: Gallstones and diabetes: an ominous
ing magnetic resonance cholangiopancreatogra- for diagnosis of Entamoeba histolytica infection. J
association. Am J Surg 102:184, 1961
phy (MRCP) at end expiration: a new technique Clin Microbiol 36:449, 1998
50. Walsh DB, Eckhauser FE, Ramsburgh SR, et al: to expand clinical application. Hepatogastroen-
Risk associated with diabetes mellitus in patients 92. Auer H, Picher O, Aspock H: Combined appli-
terology 49:593, 2002
undergoing gallbladder surgery. Surgery 91:254, cation of enzyme-linked immunosorbent assay
71. Matos C, Nicaise N, Deviere J, et al: Cho- (ELISA) and indirect haemagglutination test
1982
ledochal cysts: comparison of findings at MR (IHA) as a useful tool for the diagnosis and post-
51. Pickleman J: Controversies in biliary tract sur- cholangiopancreatography and endoscopic ret- operative surveillance of human alveolar and cys-
gery. Can J Surg 29:429, 1986 rograde cholangiopancreatography in eight pa- tic echinococcosis. Zentralbl Bakteriol Mikrobiol
52. Weissmann HS, Berkowitz D, Fox MS, et al: The tients. Radiology 209:443, 1998 Hyg [A] 270:313, 1988
role of technetium-99m iminodiacetic acid 72. Gerecht WB, Henry NK, Hoffman WW, et al: 93. Force L, Torres JM, Carrillo A, et al: Evaluation
(IDA) cholescintigraphy in acute acalculous cho- Prospective randomized comparison of mezlo- of eight serological tests in the diagnosis of
lecystitis. Radiology 146:177, 1983 cillin therapy alone with combined ampicillin human echinococcosis and follow-up. Clin Infect
53. Chen CC, Holder LE, Maunoury C, et al: Mor- and gentamicin therapy for patients with cholan- Dis 15:473, 1992
phine augmentation increases gallbladder visualiza- gitis. Arch Intern Med 149:1279, 1989
94. Aeder MI, Wellman JL, Haaga JR, et al: Role of
tion in patients pretreated with cholecystokinin. 73. Thompson JN, Edwards WH,Winearls CG, et al: surgical and percutaneous drainage in the treat-
J Nucl Med 38:644, 1997 Renal impairment following biliary tract surgery. ment of abdominal abscesses. Arch Surg 118:
54. Cabana MD, Alavi A, Berlin JA, et al: Morphine- Br J Surg 74:843, 1987 273, 1983
augmented hepatobiliary scintigraphy: a meta- 74. Thompson JE Jr, Pitt HA, Doty JE, et al: Broad 95. Ch Yu S, Hg Lo R, Kan PS, et al: Pyogenic liver
analysis. Nucl Med Commun 16:1068, 1995 spectrum penicillin as an adequate therapy for abscess: treatment with needle aspiration. Clin
55. Lo CM, Liu CL, Fan ST, et al: Prospective ran- acute cholangitis. Surg Gynecol Obstet 171:275, Radiol 52:912, 1997
domized study of early versus delayed laparo- 1990 96. Giorgio A, Tarantino L, Mariniello N, et al: Pyo-
scopic cholecystectomy for acute cholecystitis. 75. Muller EL, Pitt HA, Thompson JE Jr, et al: genic liver abscesses: 13 years of experience in
Ann Surg 227:461, 1998 Antibiotics in infections of the biliary tract. Surg percutaneous needle aspiration with US guid-
56. Koc M, Zulfikaroglu B, Kece C, et al: A prospec- Gynecol Obstet 165:285, 1987 ance. Radiology 195:122, 1995
tive randomized study of prophylactic antibiotics 76. Pitt HA, Postier RG, Cameron JL: Consequen- 97. Rajak CL, Gupta S, Jain S, et al: Percutaneous
in elective laparoscopic cholecystectomy. Surg ces of preoperative cholangitis and its treatment treatment of liver abscesses: needle aspiration
Endosc, June 17, 2003, Epub on the outcome of operation for choledocholithi- versus catheter drainage. AJR Am J Roentgenol
57. Higgins A, London J, Charland S, et al: asis. Surgery 94:447, 1983 170:1035, 1998](https://image.slidesharecdn.com/acs0818-intra-abdominalinfection-100726064008-phpapp01/75/Acs0818-Intra-Abdominal-Infection-26-2048.jpg)