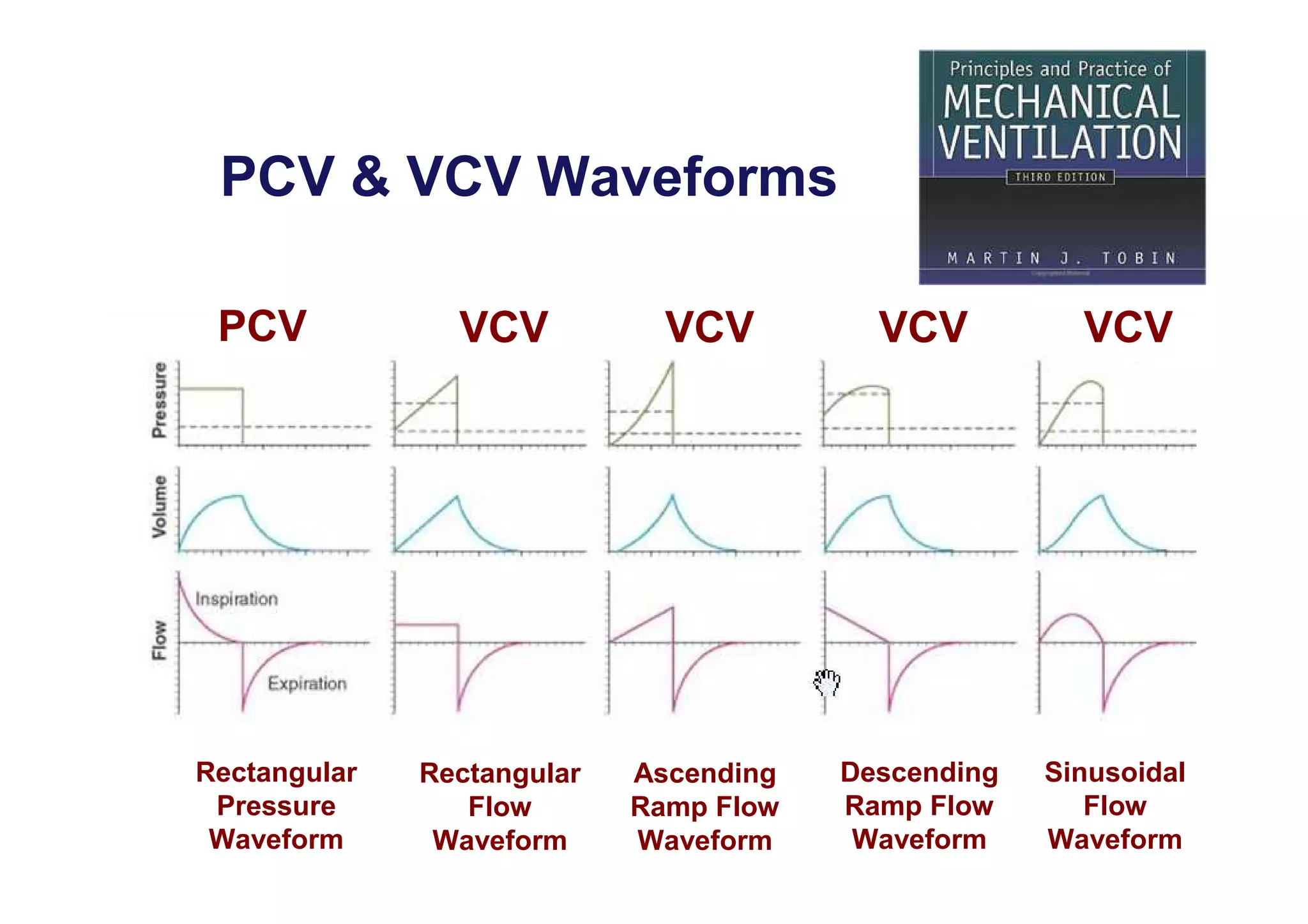
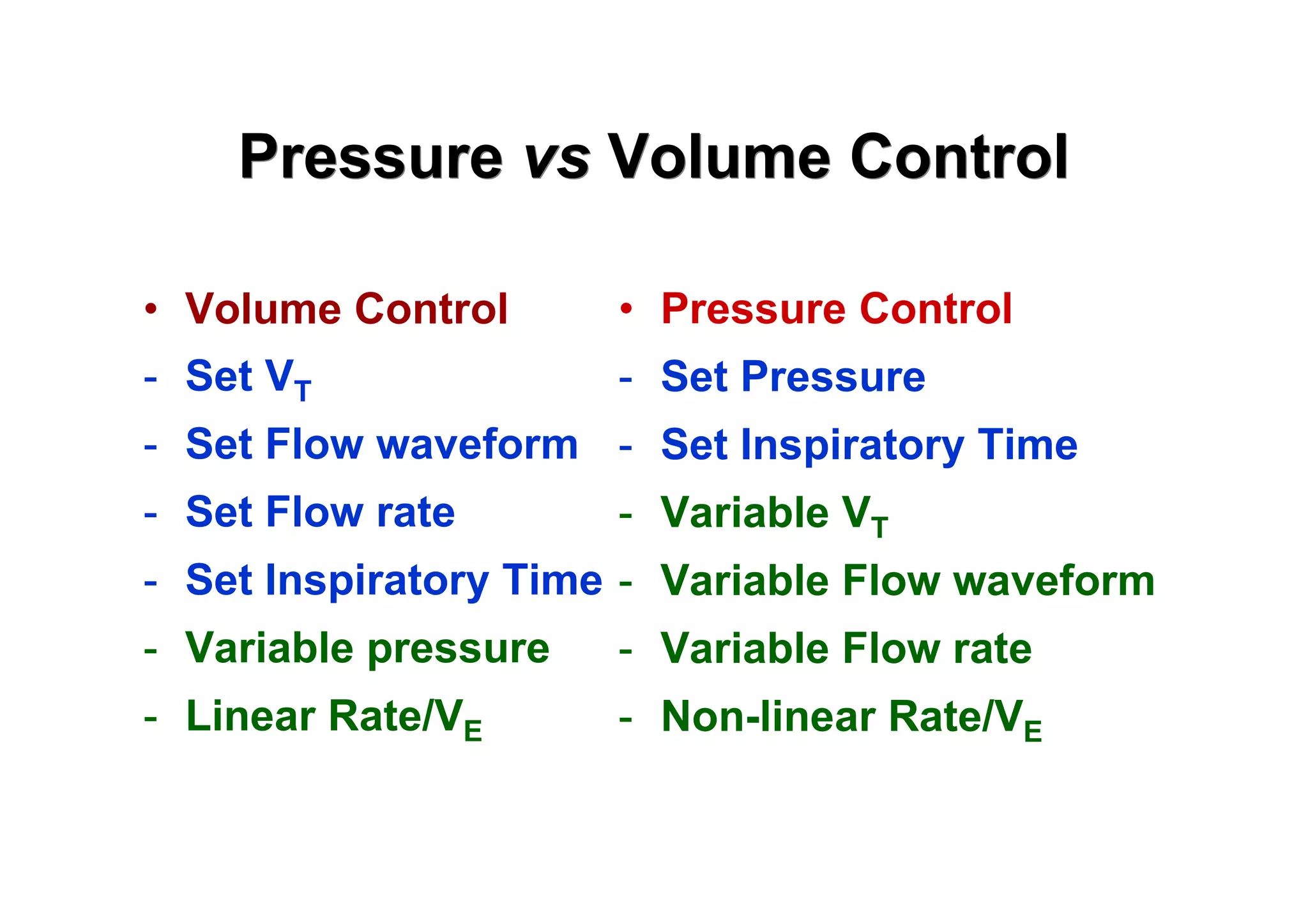
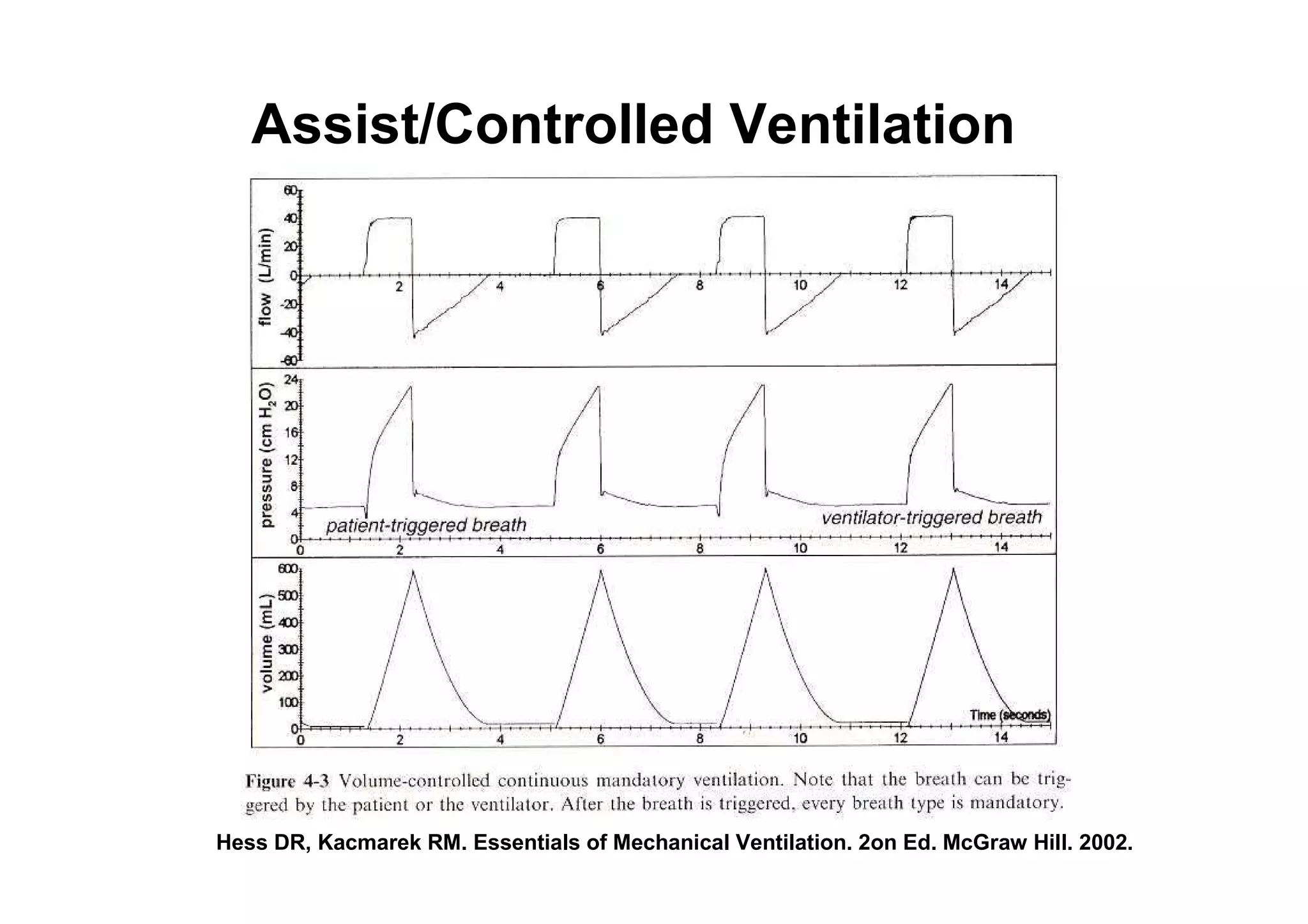
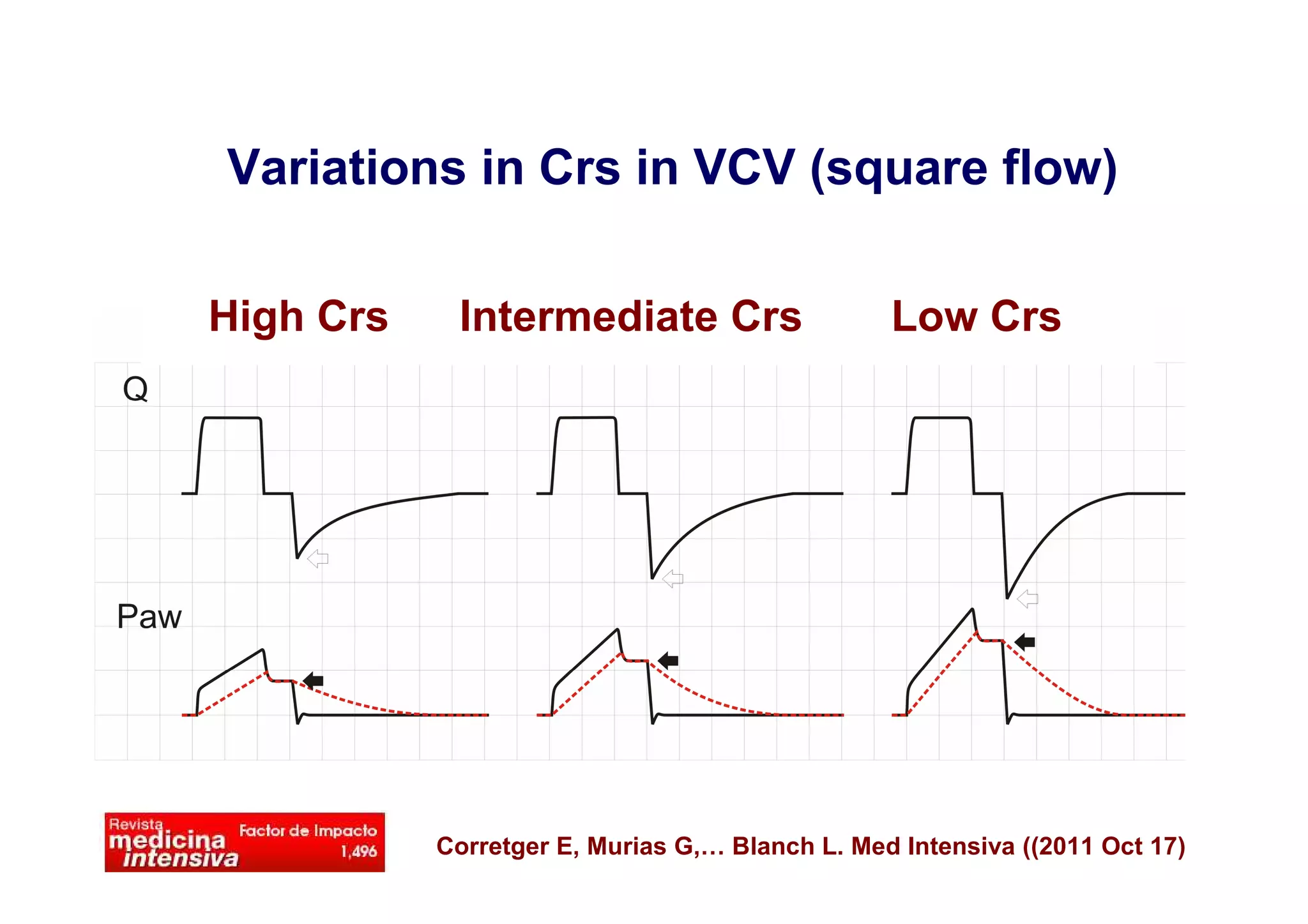
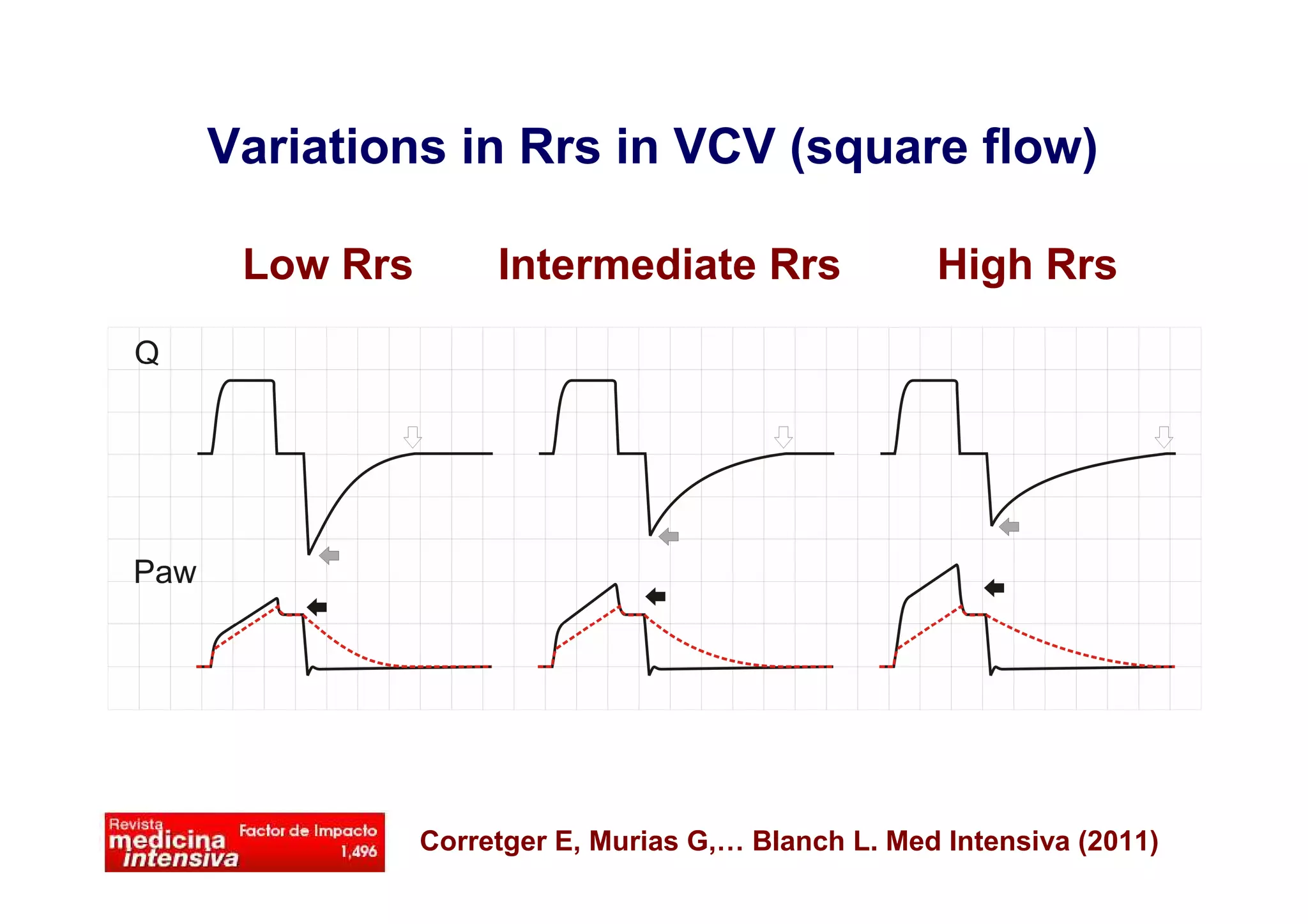
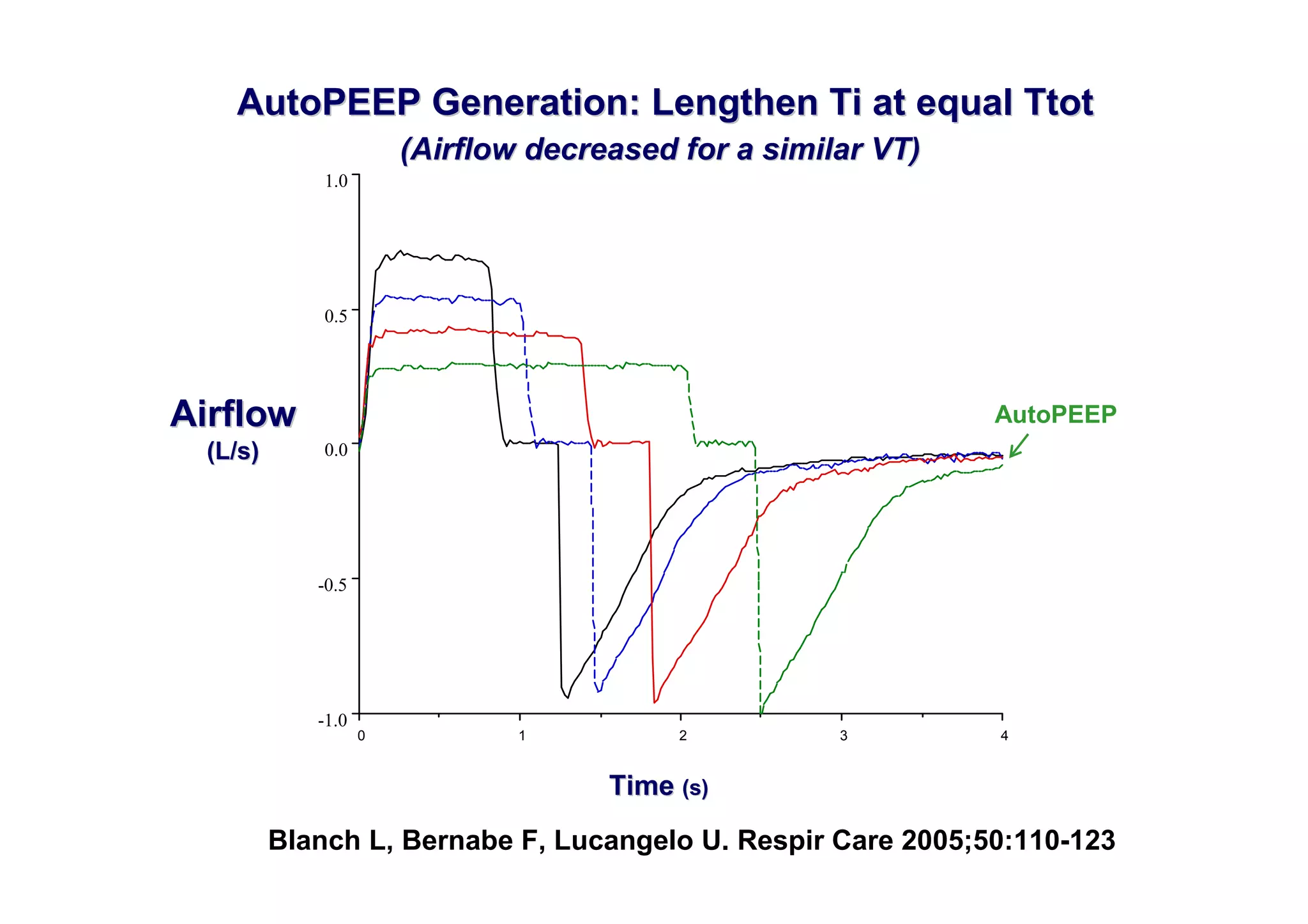
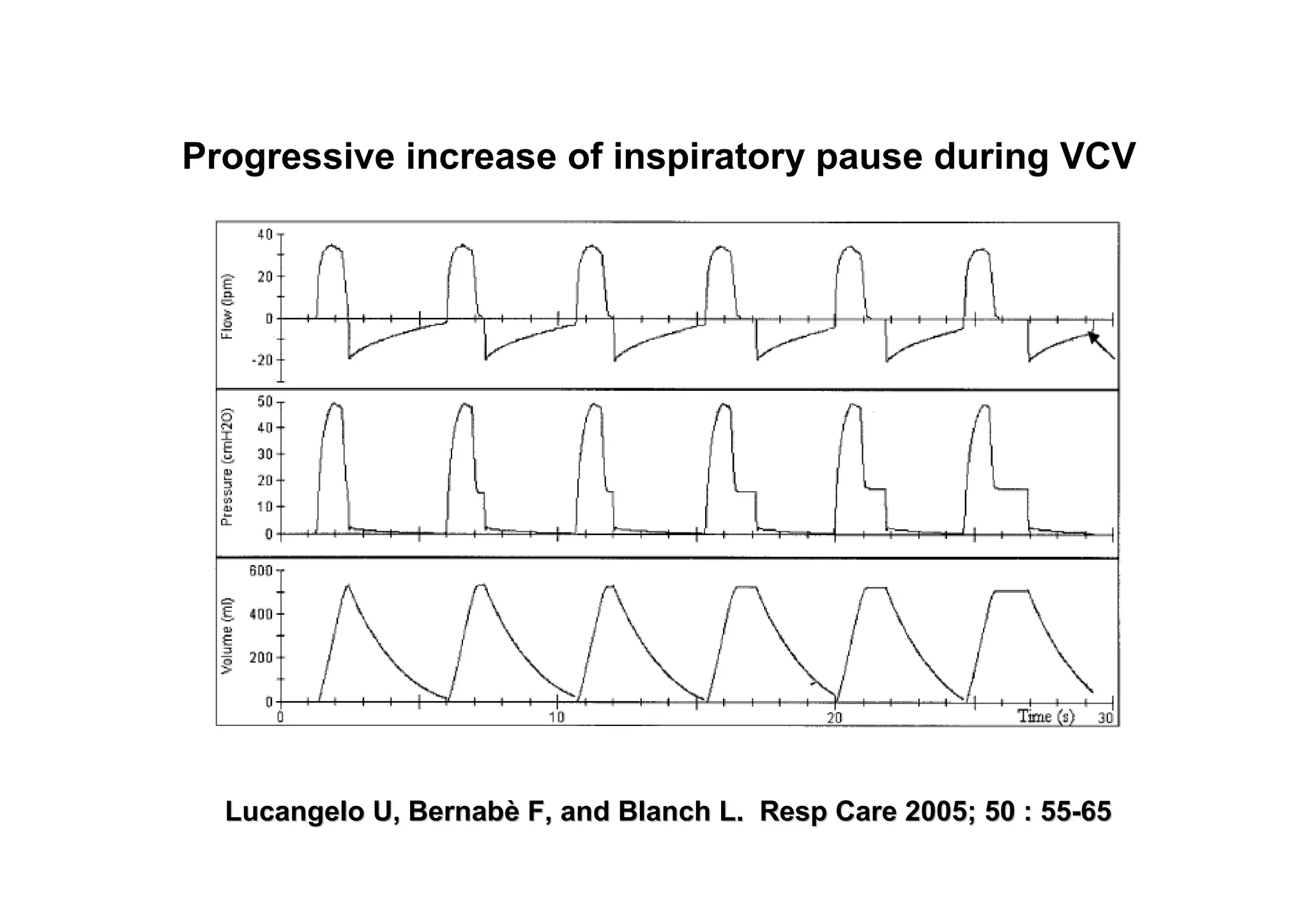

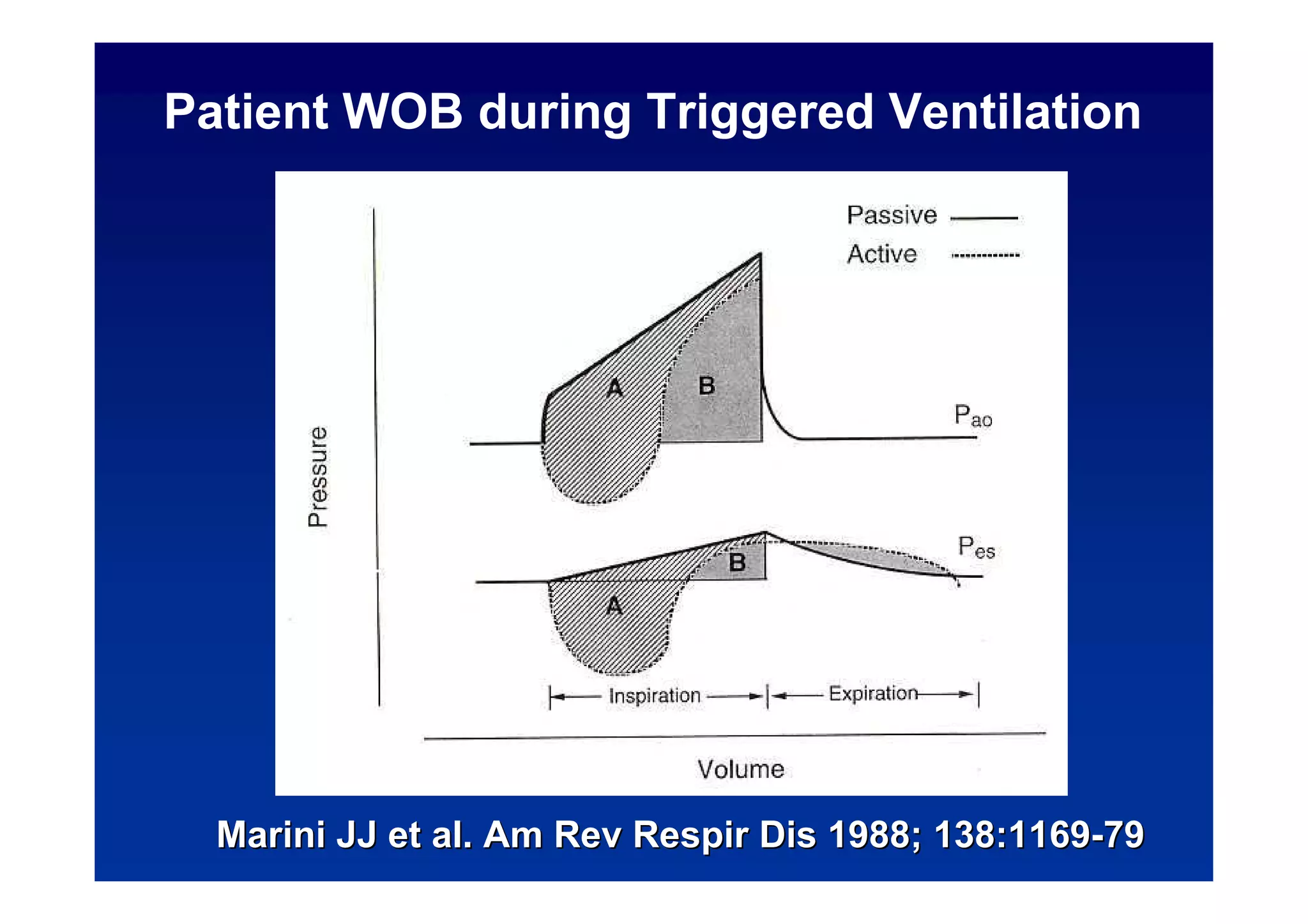
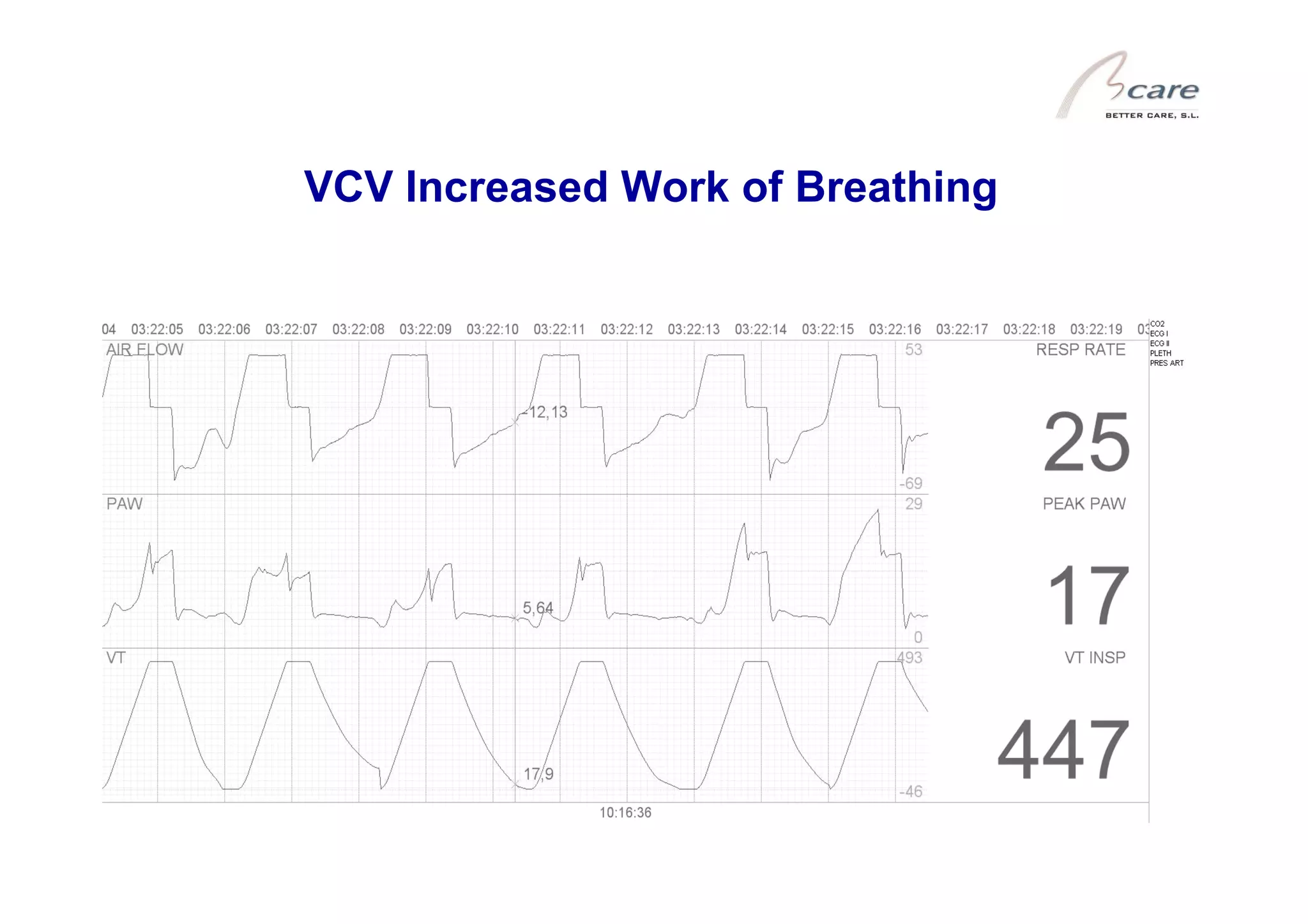
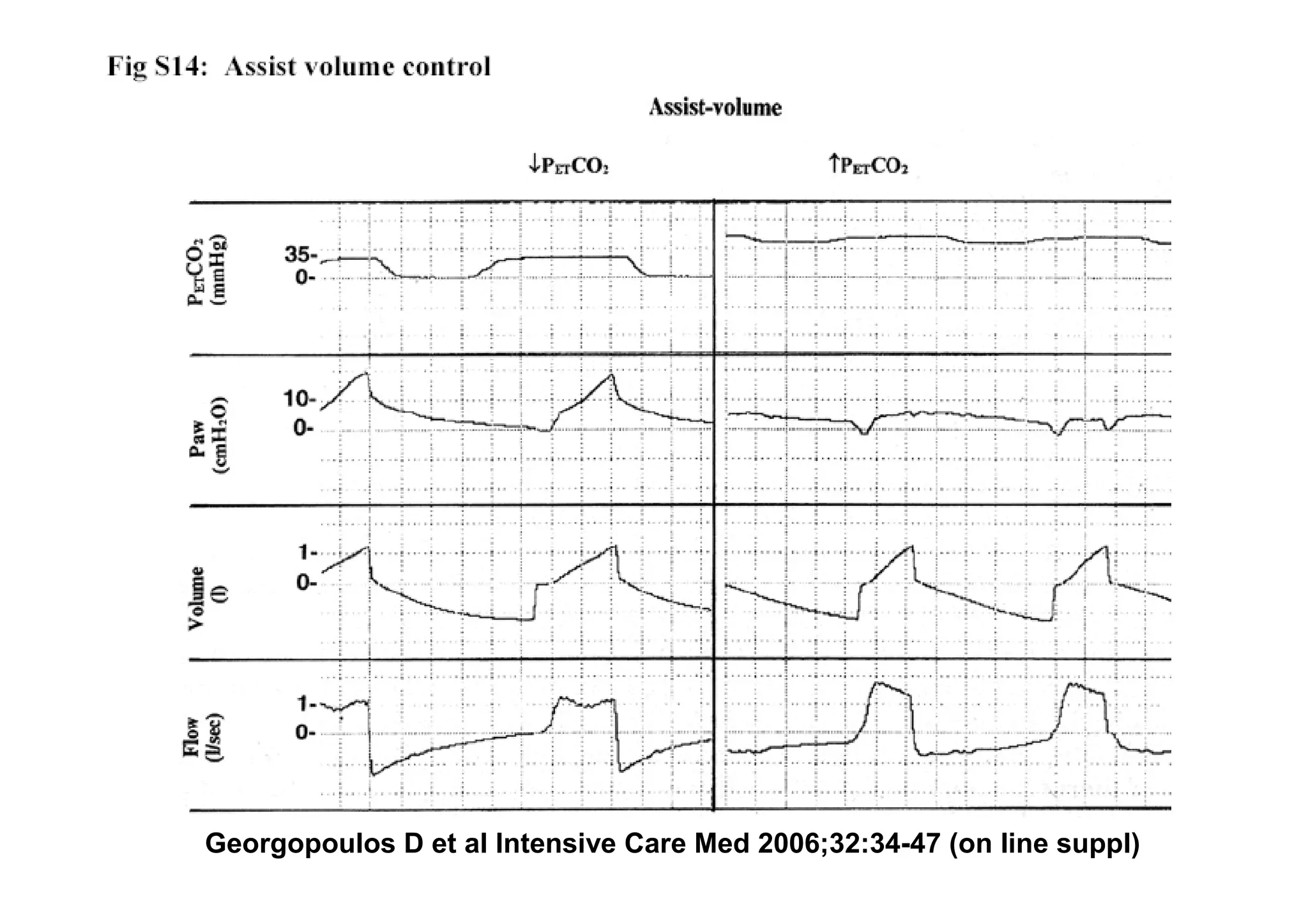
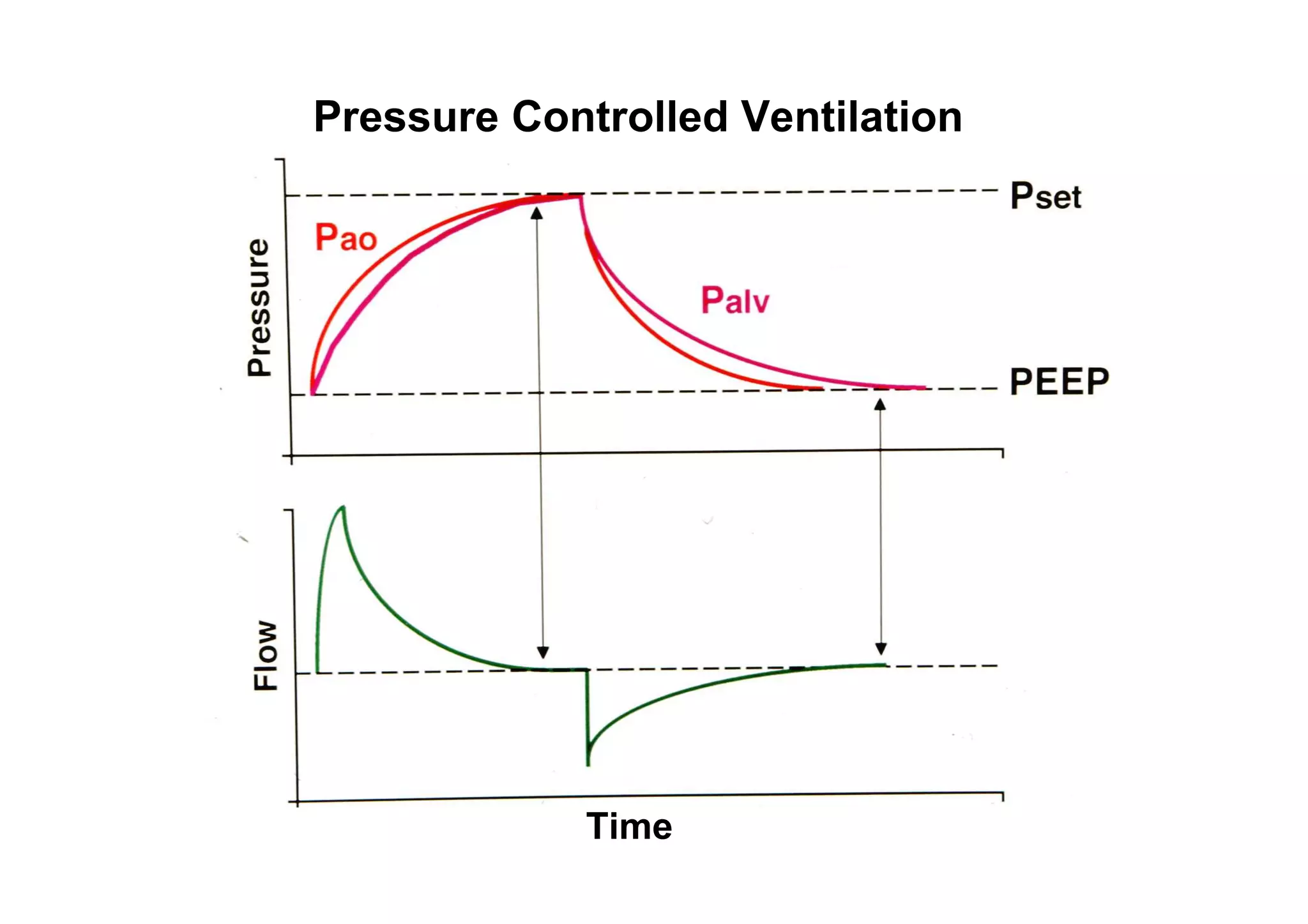
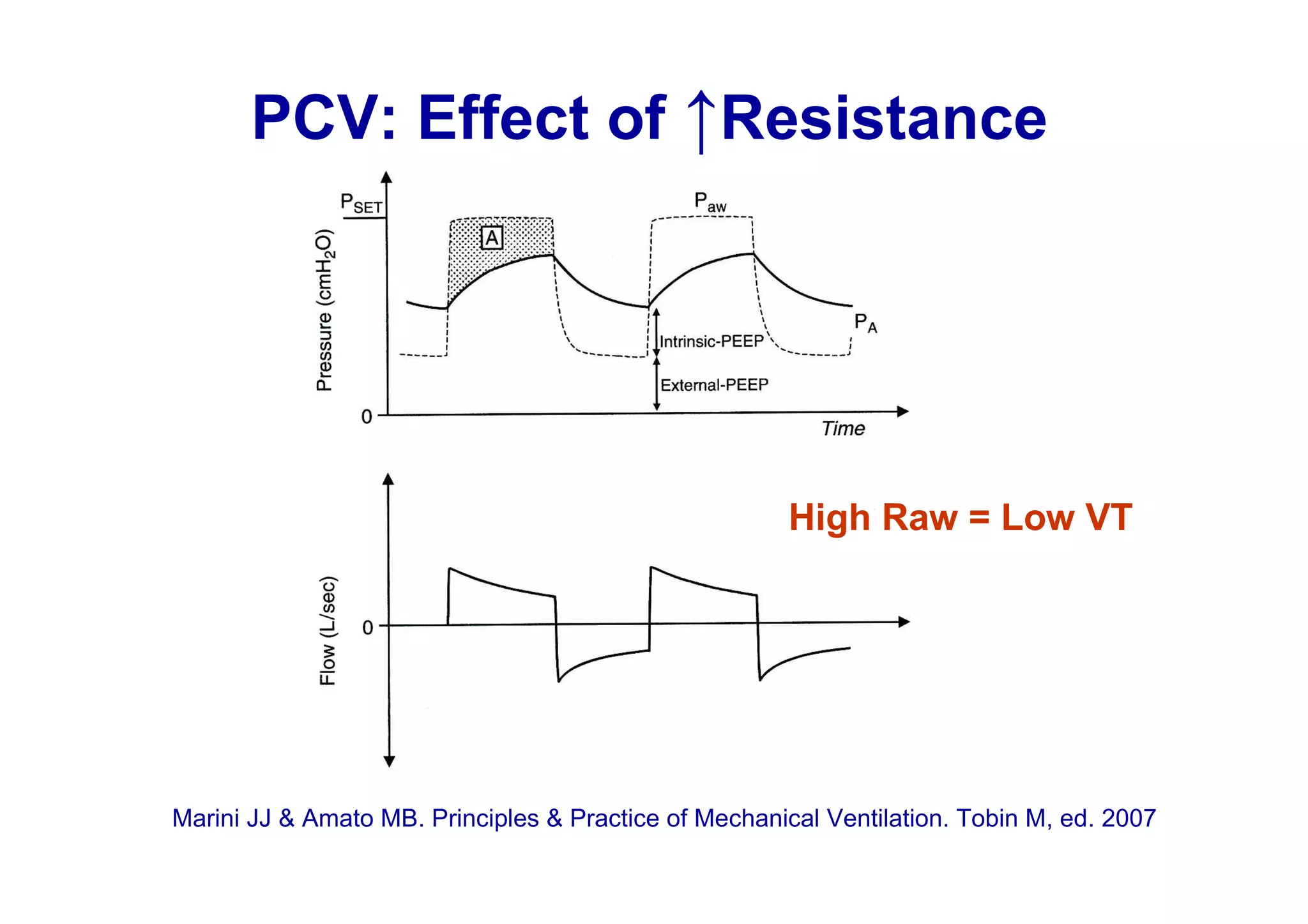
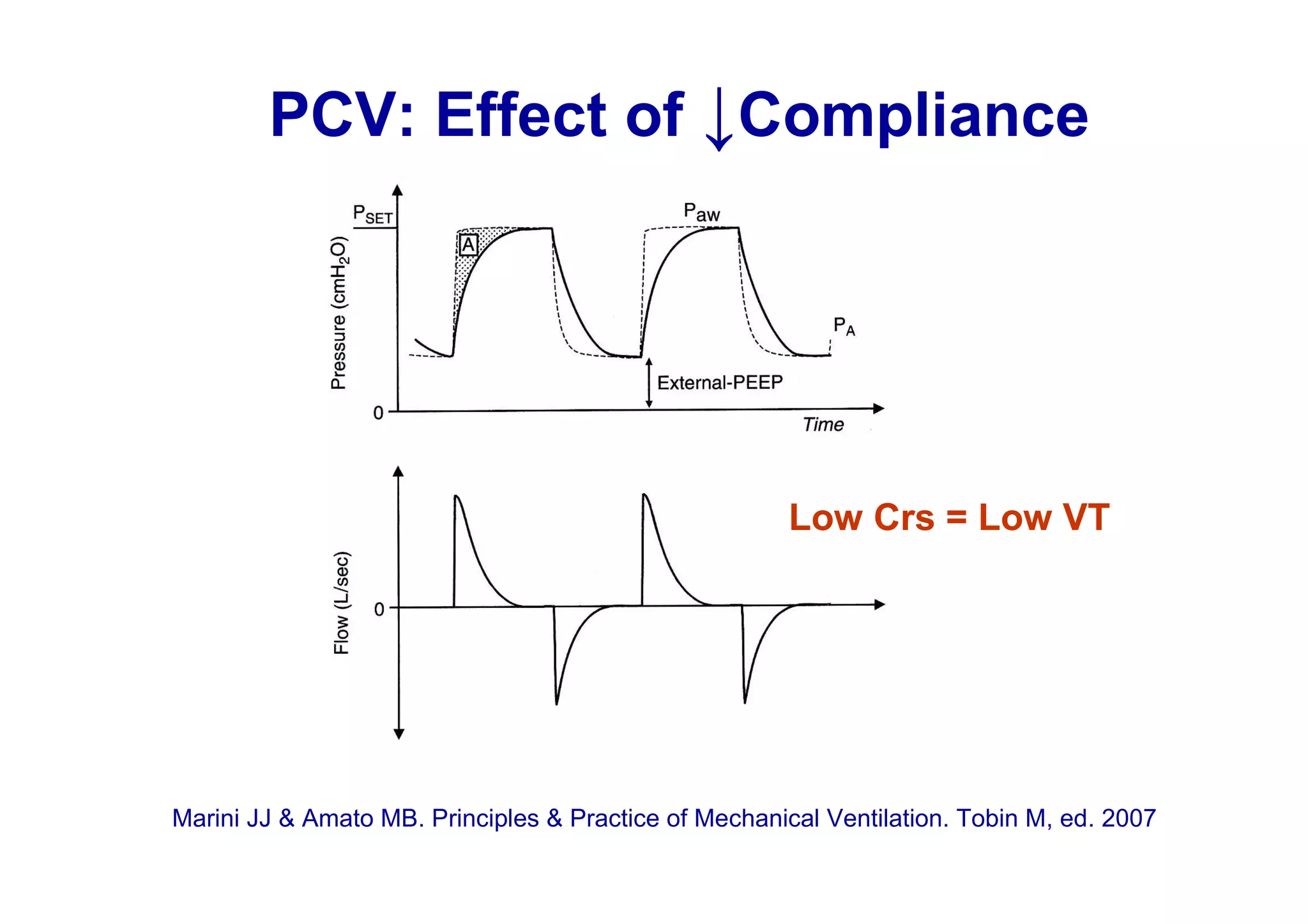
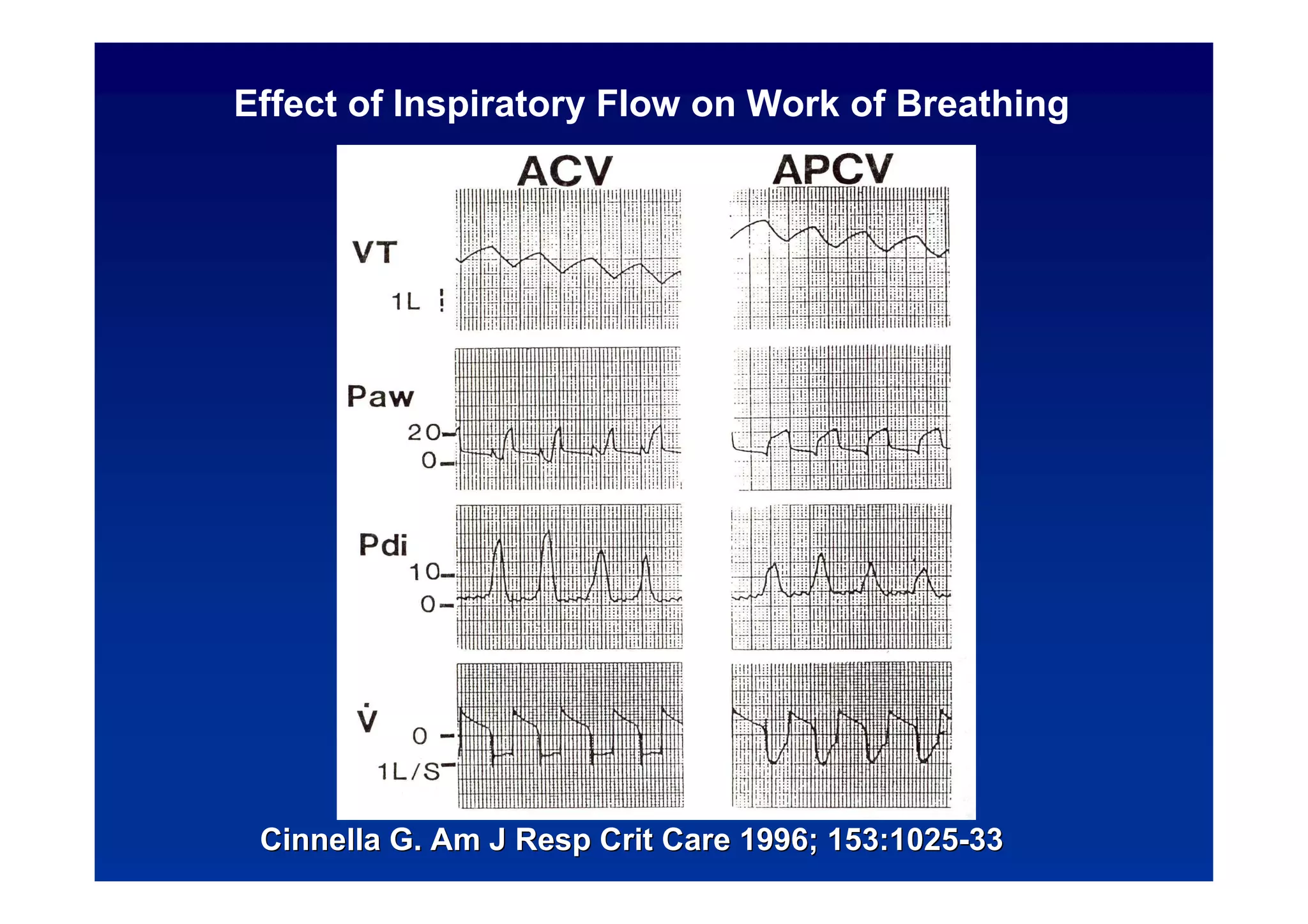
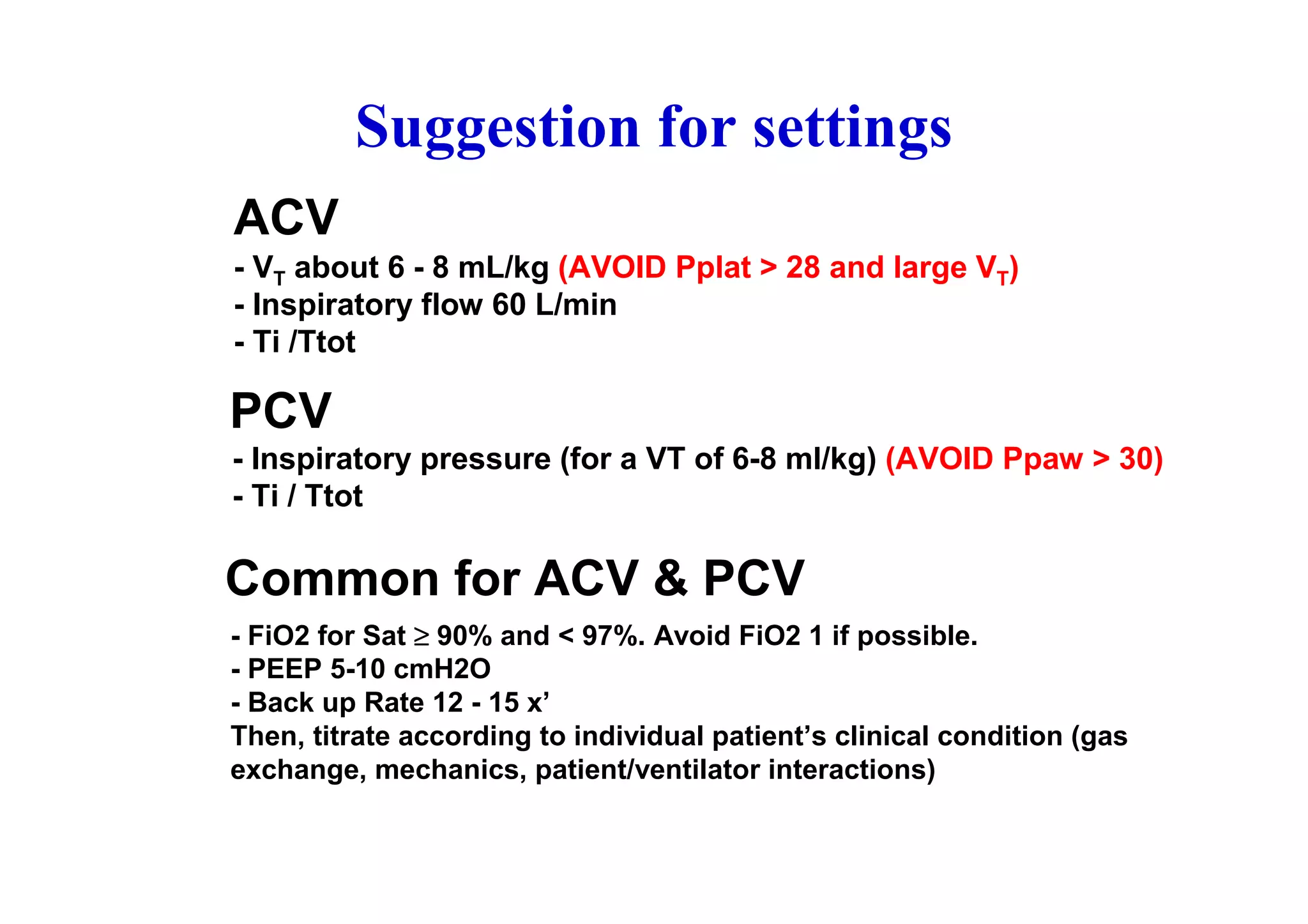
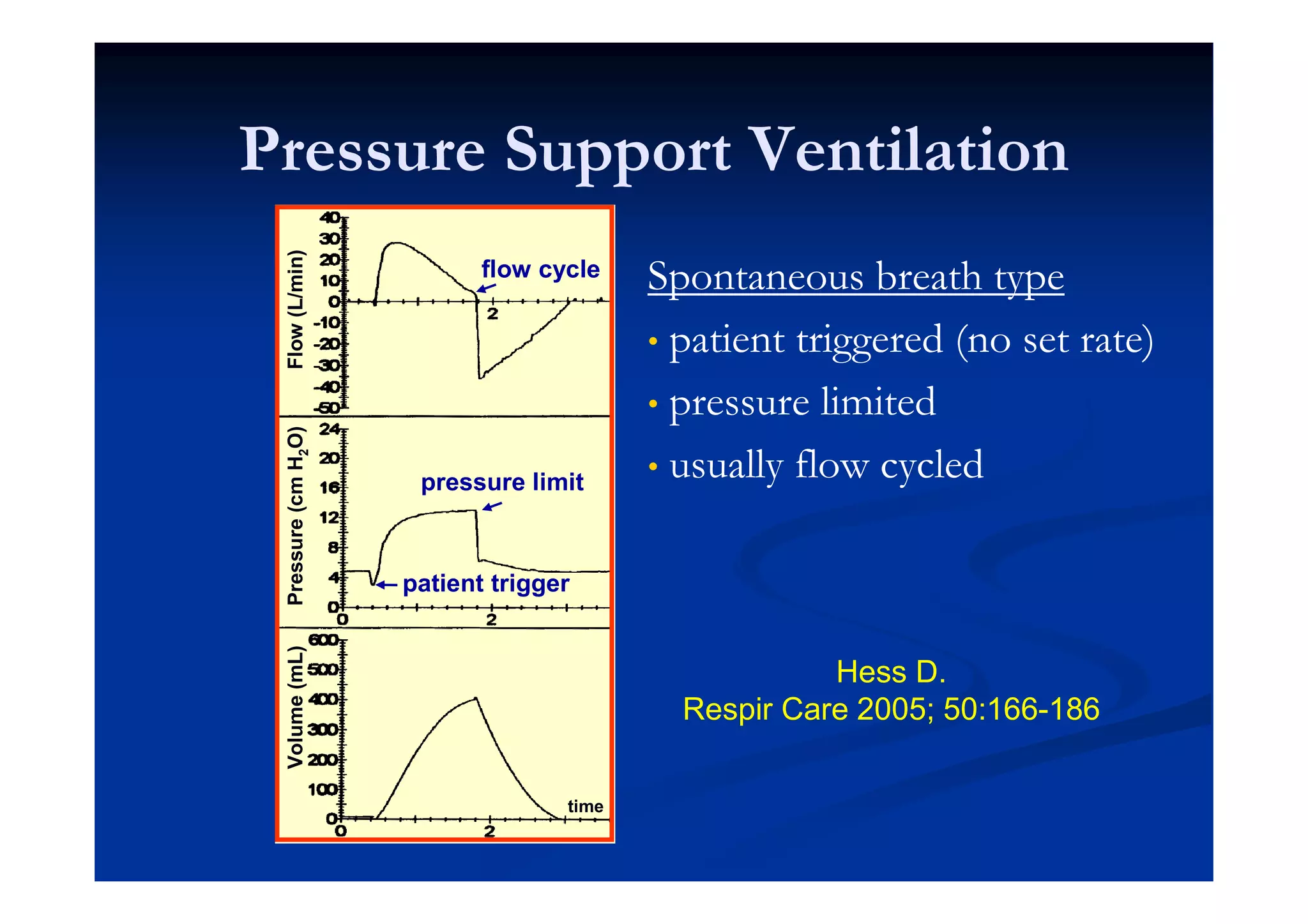
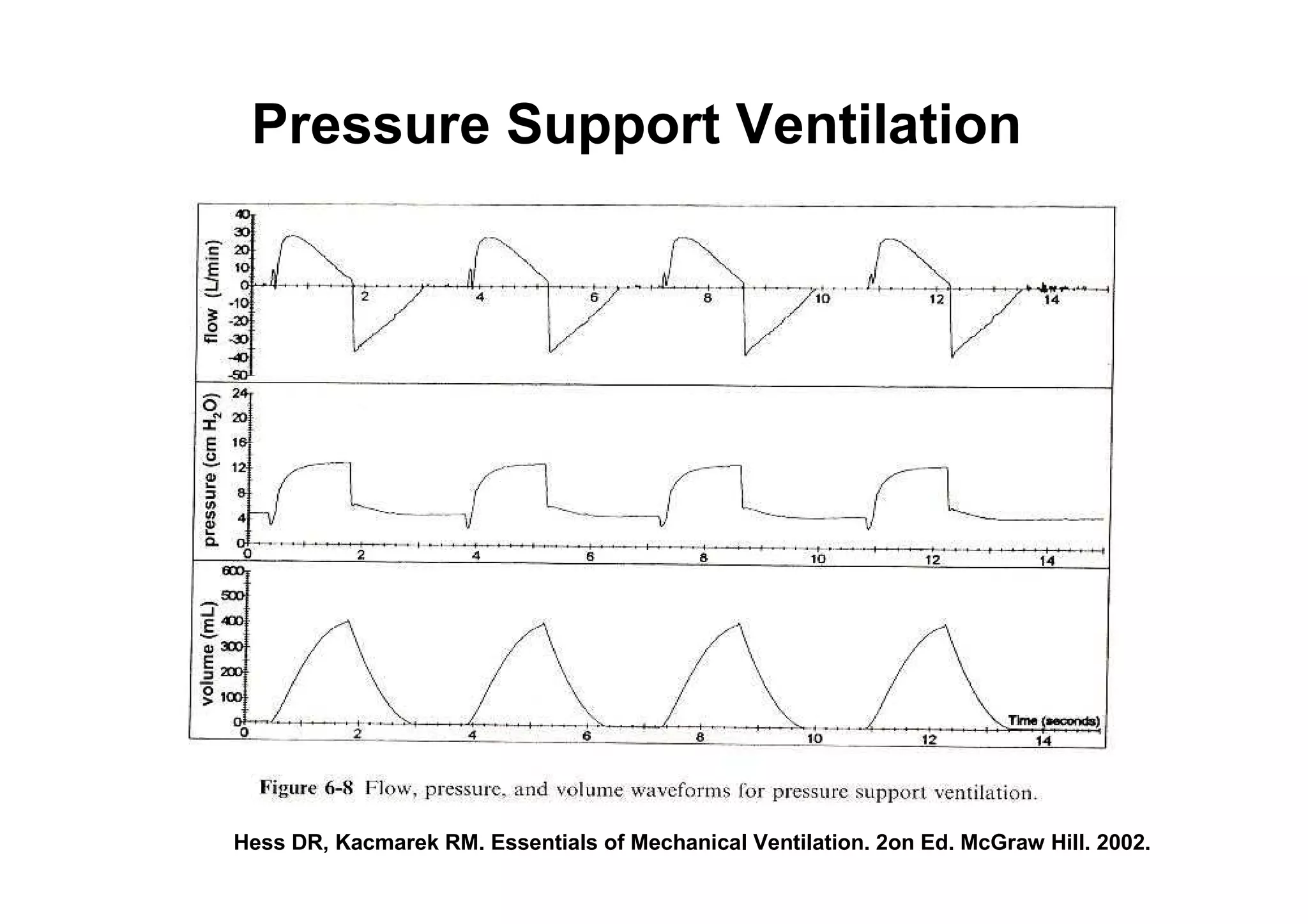
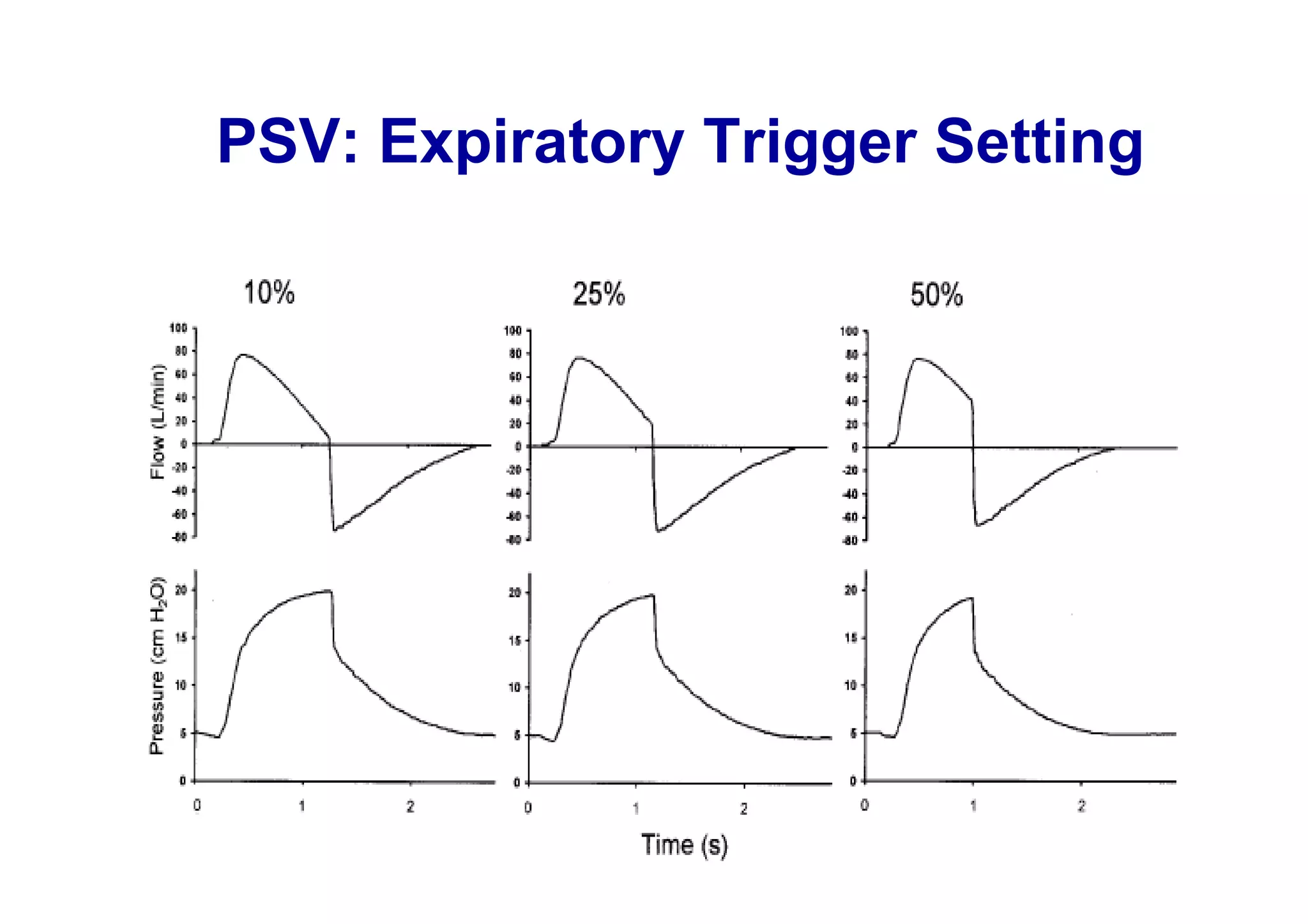
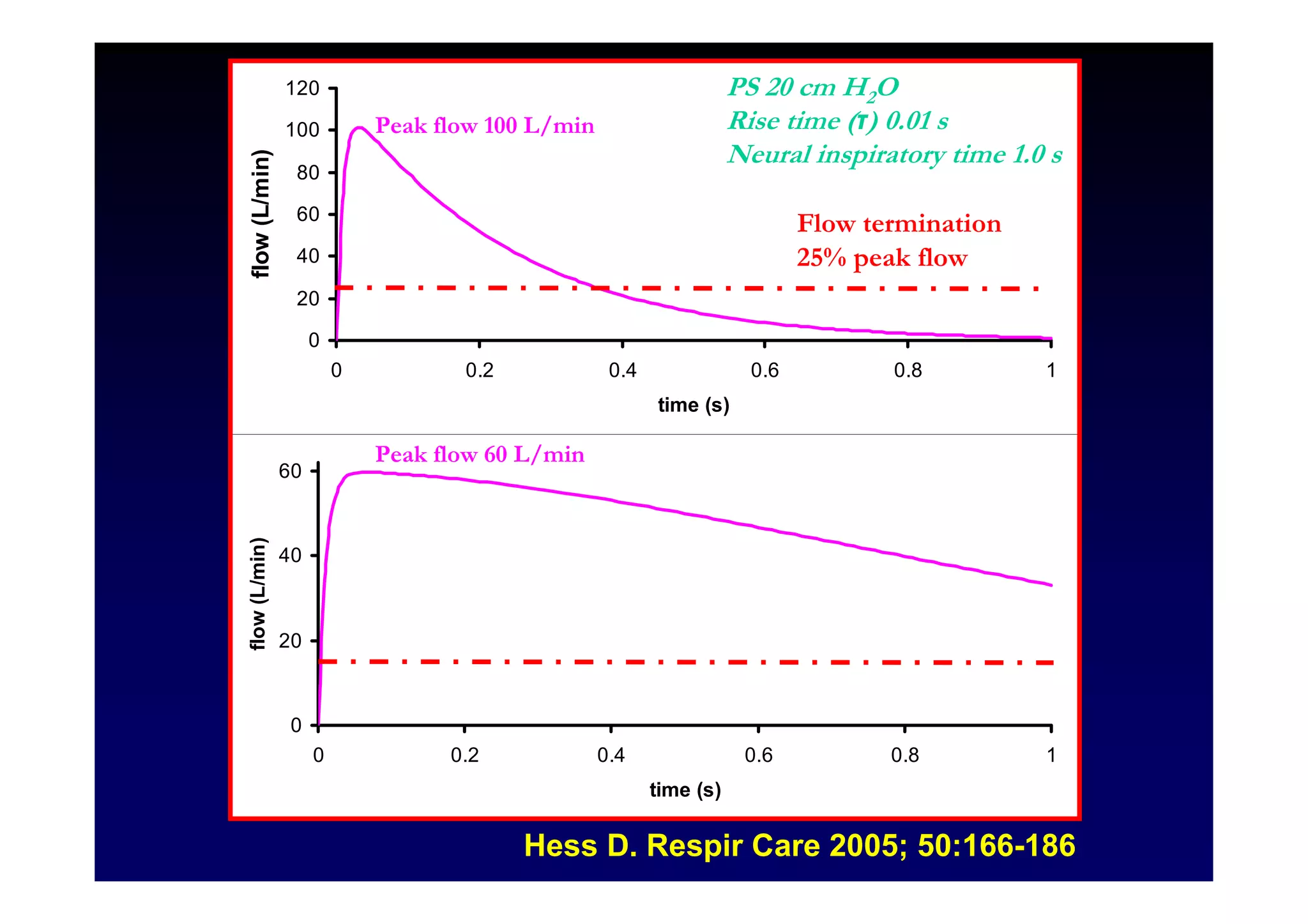
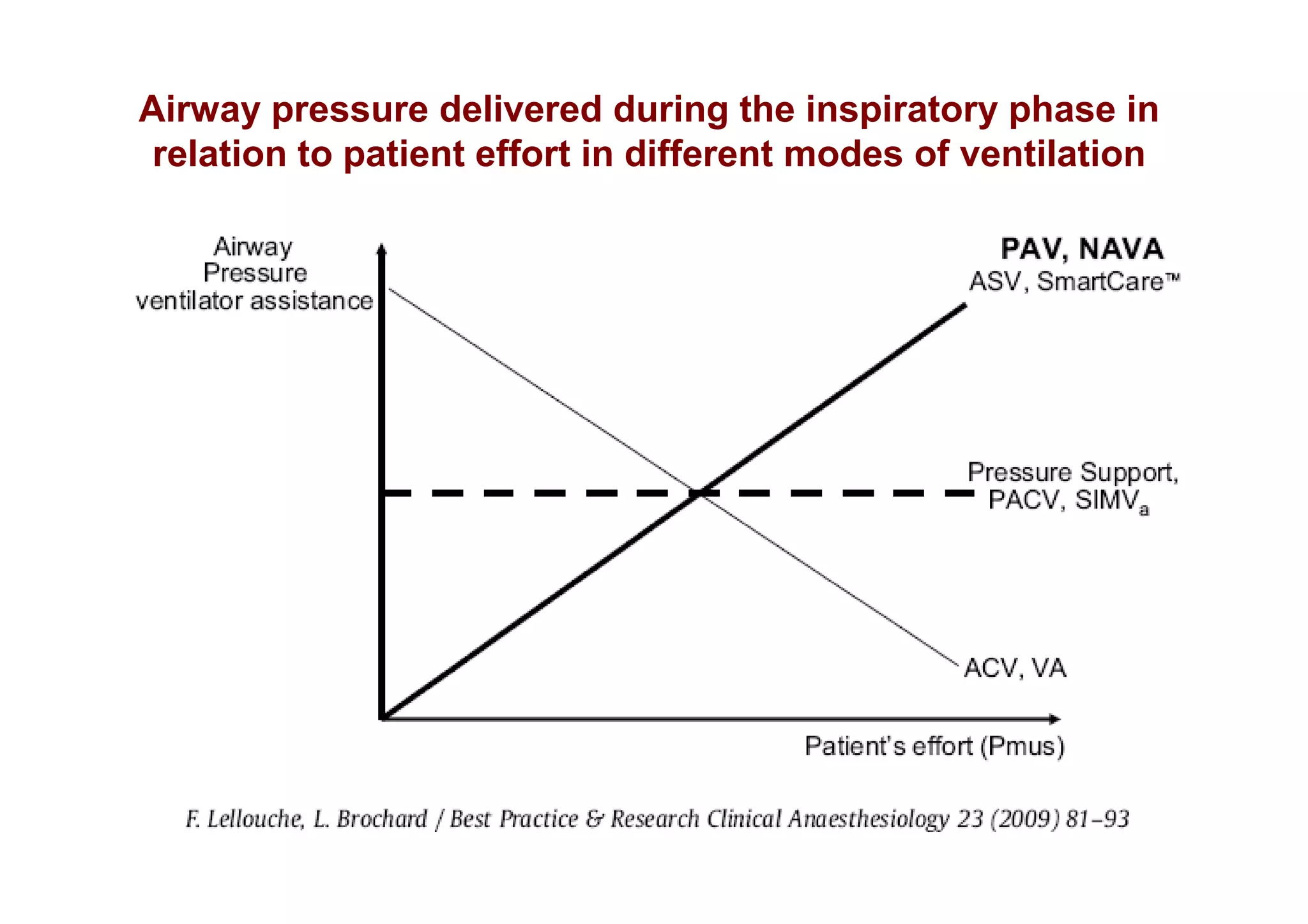

The document discusses the essential aspects of mechanical ventilation, emphasizing safety, efficacy, and patient comfort. It outlines various mechanical ventilation modes, including pressure-cycled ventilation (PCV) and volume-cycled ventilation (VCV), along with their specific variables and characteristics. The importance of clinician skills in utilizing these ventilation strategies effectively is highlighted, along with a cautionary note that new ventilator modes must be assessed critically against traditional lung-protective strategies.










































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












